

Residual ST-segment elevation to predict long-term clinical and CMR-derived outcomes in STEMI
- PMID: 36528716
- PMCID: PMC9759567
- DOI: 10.1038/s41598-022-26082-5
Residual ST-segment elevation to predict long-term clinical and CMR-derived outcomes in STEMI
Abstract
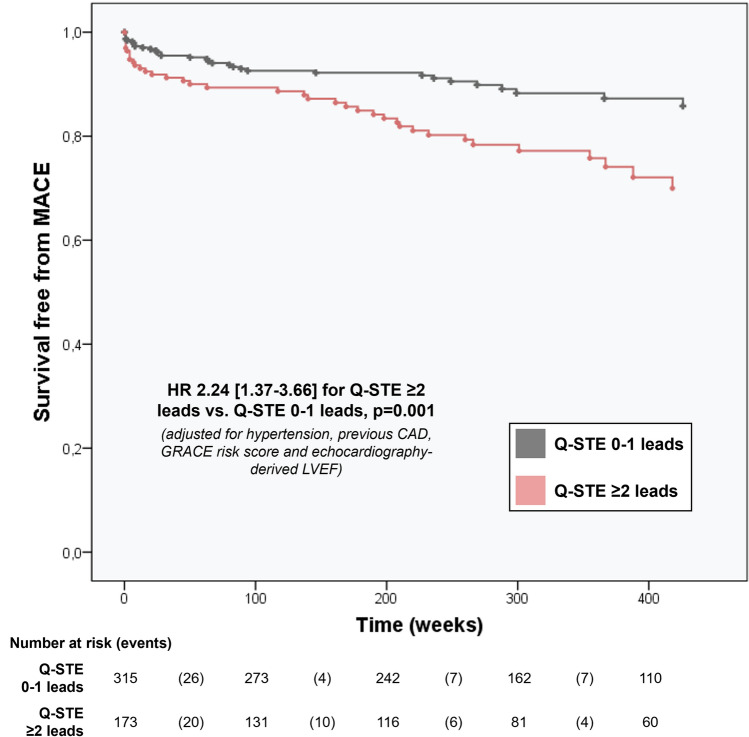
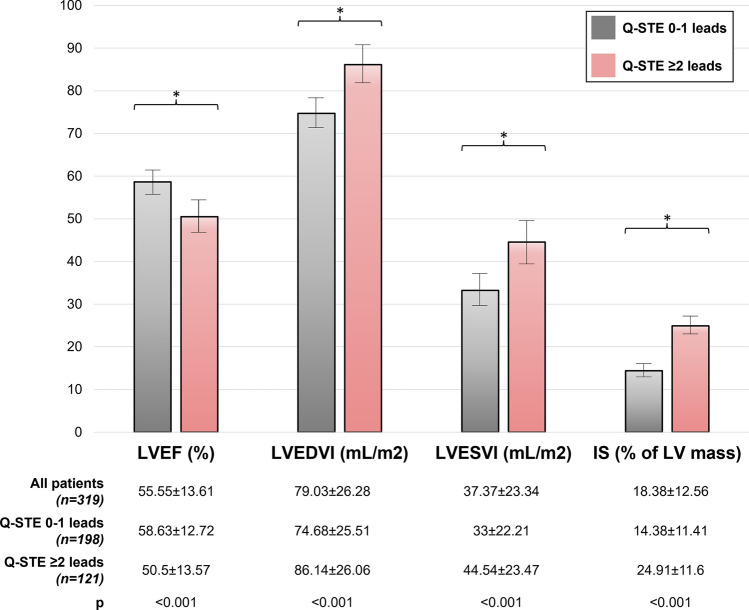
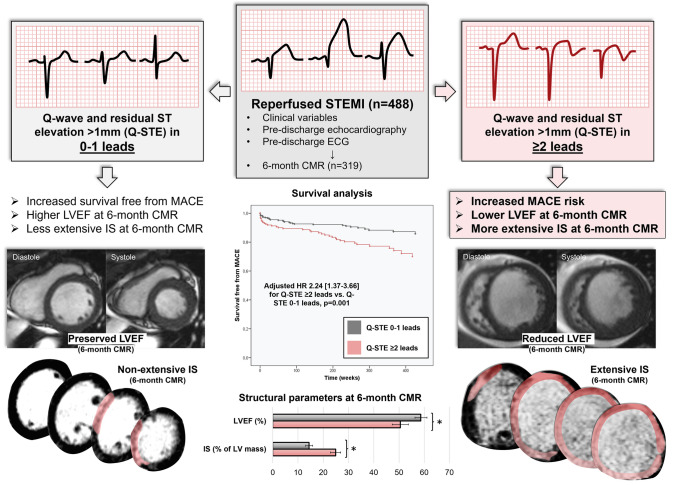
Residual ST-segment elevation after ST-segment elevation myocardial infarction (STEMI) has traditionally been considered a predictor of left ventricular (LV) dysfunction and ventricular aneurism. However, the implications in terms of long-term prognosis and cardiac magnetic resonance (CMR)-derived structural consequences are unclear. A total of 488 reperfused STEMI patients were prospectively included. The number of Q wave leads with residual ST-segment elevation > 1 mm (Q-STE) at pre-discharge ECG was assessed. LV ejection fraction (LVEF, %) and infarct size (IS, % of LV mass) were quantified in 319 patients at 6-month CMR. Major adverse cardiac events (MACE) were defined as all-cause death and/or re-admission for acute heart failure (HF), whichever occurred first. During a mean follow-up of 6.1 years, 92 MACE (18.9%), 39 deaths and 53 HF were recorded. After adjustment for baseline characteristics, Q-STE (per lead with > 1 mm) was independently associated with a higher risk of long-term MACE (HR 1.24 [1.07-1.44] per lead, p = 0.004), reduced (< 40%) LVEF (HR 1.36 [1.02-1.82] per lead, p = 0.04) and large (> 30% of LV mass) IS (HR 1.43 [1.11-1.85] per lead, p = 0.006) at 6-month CMR. Patients with Q-STE ≥ 2 leads (n = 172, 35.2%) displayed lower MACE-free survival, more depressed LVEF, and larger IS at 6-month CMR (p < 0.001 for all comparisons). Residual ST-segment elevation after STEMI represents a universally available tool that predicts worse long-term clinical and CMR-derived structural outcomes.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
