

ARDS: hidden perils of an overburdened diagnosis
- PMID: 36528765
- PMCID: PMC9758457
- DOI: 10.1186/s13054-022-04271-y
ARDS: hidden perils of an overburdened diagnosis
Abstract
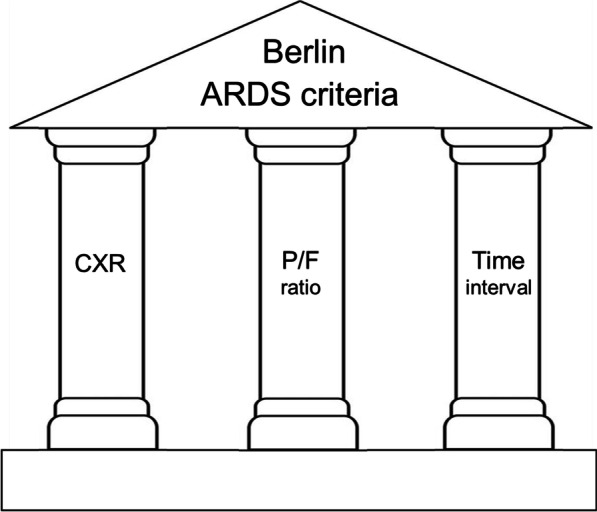
A diagnosis of ARDS serves as a pretext for several perilous clinical practices. Clinical trials demonstrated that tidal volume 12 ml/kg increases patient mortality, but 6 ml/kg has not proven superior to 11 ml/kg or anything in between. Present guidelines recommend 4 ml/kg, which foments severe air hunger, leading to prescription of hazardous (yet ineffective) sedatives, narcotics and paralytic agents. Inappropriate lowering of tidal volume also fosters double triggering, which promotes alveolar overdistention and lung injury. Successive panels have devoted considerable energy to developing a more precise definition of ARDS to homogenize the recruitment of patients into clinical trials. Each of three pillars of the prevailing Berlin definition is extremely flimsy and the source of confusion and unscientific practices. For doctors at the bedside, none of the revisions have enhanced patient care over that using the original 1967 description of Ashbaugh and colleagues. Bedside doctors are better advised to diagnose ARDS on the basis of pattern recognition and instead concentrate their vigilance on resolving the numerous hidden dangers that follow inevitably once a diagnosis has been made.
© 2022. The Author(s).
Conflict of interest statement
My Competing interests are that I receive royalties for two books on critical care published by McGraw-Hill, Inc., New York.
Figures
References
-
- Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi-Filho G, Kairalla RA, Deheinzelin D, Munoz C, Oliveira R, Takagaki TY, Carvalho CR. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome. N Engl J Med. 1998;338(6):347–354. doi: 10.1056/NEJM199802053380602. - DOI - PubMed
-
- Acute Respiratory Distress Syndrome Network, Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, Wheeler A. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000;342(18):1301–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
