

Insights into Sickle Cell Disease through the Retinal Microvasculature: Adaptive Optics Scanning Light Ophthalmoscopy Correlates of Clinical OCT Angiography
- PMID: 36531581
- PMCID: PMC9754983
- DOI: 10.1016/j.xops.2022.100196
Insights into Sickle Cell Disease through the Retinal Microvasculature: Adaptive Optics Scanning Light Ophthalmoscopy Correlates of Clinical OCT Angiography
Abstract
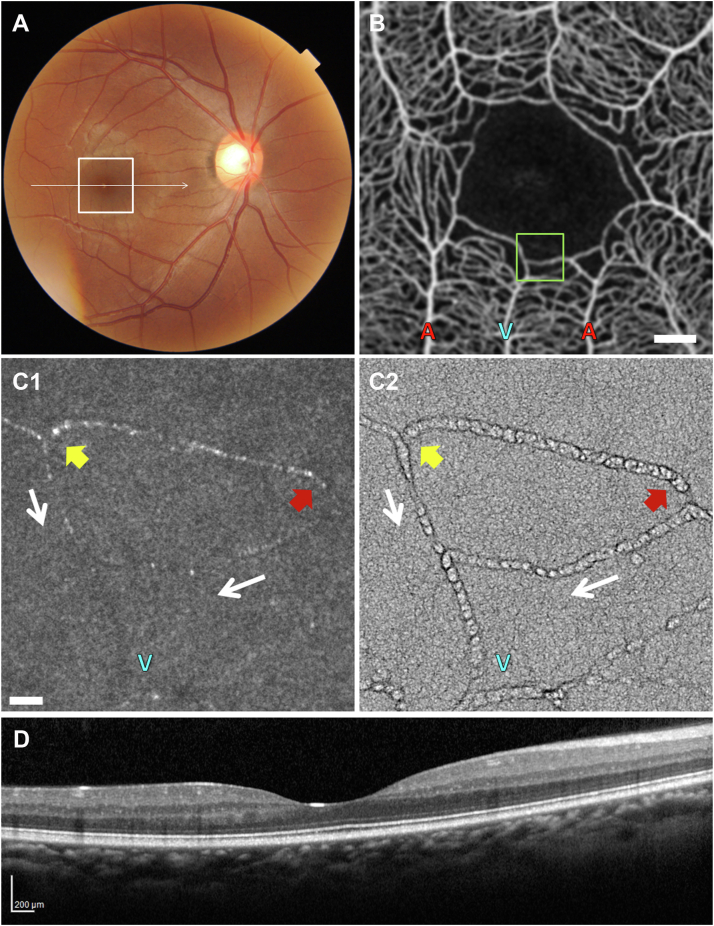
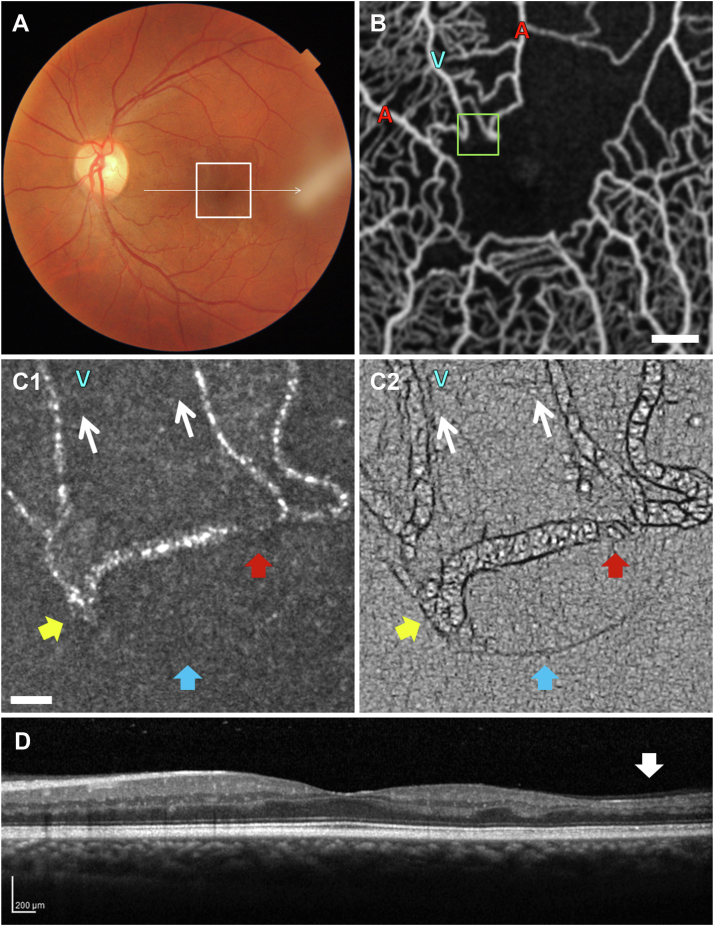
Purpose: Clinical OCT angiography (OCTA) of the retinal microvasculature offers a quantitative correlate to systemic disease burden and treatment efficacy in sickle cell disease (SCD). The purpose of this study was to use the higher resolution of adaptive optics scanning light ophthalmoscopy (AOSLO) to elucidate OCTA features of parafoveal microvascular compromise identified in SCD patients.
Design: Case series of 11 SCD patients and 1 unaffected control.
Participants: A total of 11 eyes of 11 SCD patients (mean age, 33 years; range, 23-44; 8 female, 3 male) and 1 eye of a 34-year-old unaffected control.
Methods: Ten sequential 3 × 3 mm parafoveal OCTA full vascular slab scans were obtained per eye using a commercial spectral domain OCT system (Avanti RTVue-XR; Optovue). These were used to identify areas of compromised perfusion near the foveal avascular zone (FAZ), designated as regions of interest (ROIs). Immediately thereafter, AOSLO imaging was performed on these ROIs to examine the cellular details of abnormal perfusion. Each participant was imaged at a single cross-sectional time point. Additionally, 2 of the SCD patients were imaged prospectively 2 months after initial imaging to study compromised capillary segments across time and with treatment.
Main outcome measures: Detection and characterization of parafoveal perfusion abnormalities identified using OCTA and resolved using AOSLO imaging.
Results: We found evidence of abnormal blood flow on OCTA and AOSLO imaging among all 11 SCD patients with diverse systemic and ocular histories. Adaptive optics scanning light ophthalmoscopy imaging revealed a spectrum of phenomena, including capillaries with intermittent blood flow, blood cell stasis, and sites of thrombus formation. Adaptive optics scanning light ophthalmoscopy imaging was able to resolve single sickled red blood cells, rouleaux formations, and blood cell-vessel wall interactions. OCT angiography and AOSLO imaging were sensitive enough to document improved retinal perfusion in an SCD patient 2 months after initiation of oral hydroxyurea therapy.
Conclusions: Adaptive optics scanning light ophthalmoscopy imaging was able to reveal the cellular details of perfusion abnormalities detected using clinical OCTA. The synergy between these clinical and laboratory imaging modalities presents a promising avenue in the management of SCD through the development of noninvasive ocular biomarkers to prognosticate progression and measure the response to systemic treatment.
Keywords: ADD, airy disk diameter; AOSLO, adaptive optics scanning light ophthalmoscopy; Adaptive optics; BCVA, best-corrected visual acuity; D, diopters; FA, fluorescein angiography; FAZ, foveal avascular zone; HbSC, hemoglobin SC; HbSS, hemoglobin SS; IOP, intraocular pressure; OCT angiography; OCTA, OCT angiography; Oculomics; RBC, red blood cell; ROI, region of interest; Retinal microvasculature; SCD, sickle cell disease; SCR, sickle cell retinopathy; Sickle cell disease.
© 2022 by the American Academy of Ophthalmology.
Figures






References
-
- Kato G.J., Piel F.B., Reid C.D., et al. Sickle cell disease. Nat Rev Dis Primers. 2018;4 - PubMed
-
- Hassell K.L. Population estimates of sickle cell disease in the U.S. Am J Prev Med. 2010;38(4 Suppl):S512–S521. - PubMed
-
- Dina S. Cost of illness of sickle cell disease in the US, payers’ perspective: (CRESCENT). Poster presentation at Virtual ISPOR 2021. May 17-20, 2021.
Grants and funding
LinkOut - more resources
Full Text Sources
