

A Rare Case of a Prostatic Abscess Secondary to a Mycoplasma hominis Infection
- PMID: 36532918
- PMCID: PMC9750243
- DOI: 10.7759/cureus.31491
A Rare Case of a Prostatic Abscess Secondary to a Mycoplasma hominis Infection
Abstract
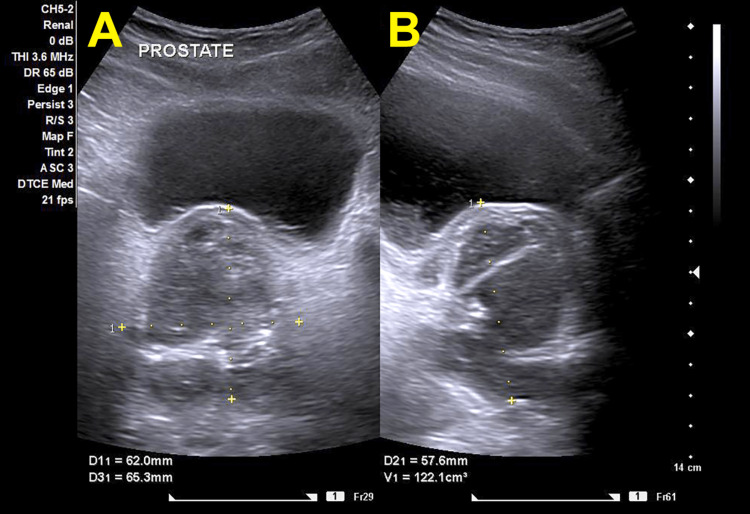
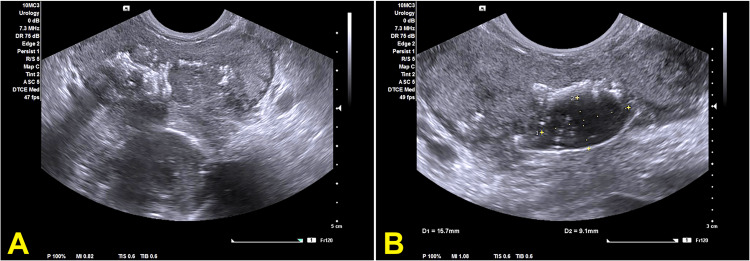
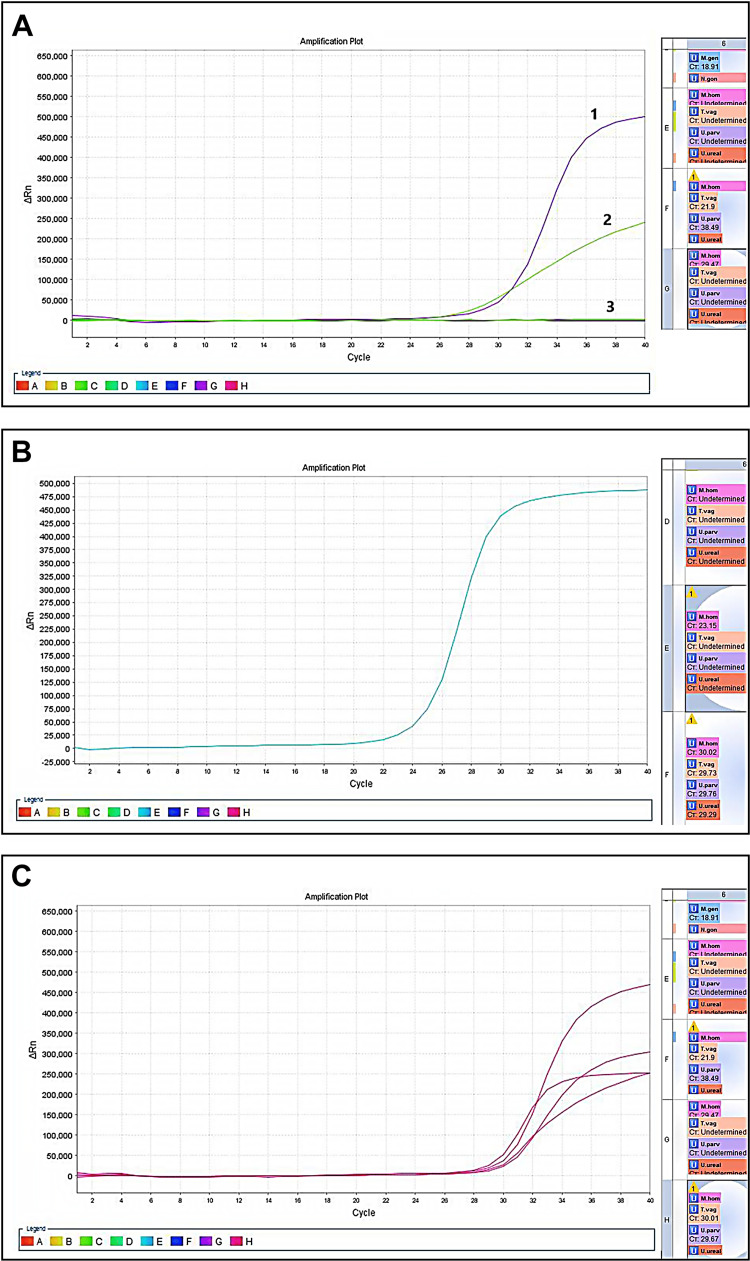
Mycoplasma hominis is one of the pathogenic organisms that may cause prostatitis with the development of a prostatic abscess in very rare cases. A 57-year-old man presented with lower urinary tract symptoms and low-grade fever. The transabdominal ultrasonography showed prostate enlargement suggesting acute prostatitis. The patient was started on empiric antibacterial therapy with fluoroquinolones. The urine and semen cultures showed no bacterial growth. A few days later, the patient presented again with symptoms progression and acute urinary retention. The transrectal ultrasound revealed diffuse calcifications and intraprostatic fluids. The computed tomography of the abdomen and pelvis showed a large abscess in the prostate with a periprostatic inflammatory reaction. While all bacterial cultures were negative, the multiplex polymerase chain reaction (PCR) test revealed a Mycoplasma hominis infection. The patient was managed with transurethral drainage. After six months of follow-up, the patient was free of symptoms and the repeat PCR study confirmed clearance of the Mycoplasma infection.
Keywords: acute prostatitis; multiplex pcr; mycoplasma hominis; mycoplasma infections; pcr multiplex; prostate abscess; prostate surgery; prostatic abscess; transrectal ultrasound scan; transurethral drainage.
Copyright © 2022, Jagtap et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Prostatic abscess: diagnosis and treatment. Barozzi L, Pavlica P, Menchi I, De Matteis M, Canepari M. AJR Am J Roentgenol. 1998;170:753–757. - PubMed
-
- The 2001 Giessen Cohort Study on patients with prostatitis syndrome--an evaluation of inflammatory status and search for microorganisms 10 years after a first analysis. Schneider H, Ludwig M, Hossain HM, Diemer T, Weidner W. Andrologia. 2003;35:258–262. - PubMed
-
- Treatment strategy for prostatic abscess: eighteen cases' report and review of literature. Oshinomi K, Matsui Y, Unoki T, et al. Urol Sci. 2018;29:206–209.
-
- Prostatic abscess: diagnosis and treatment of an infrequent urological entity (Article in Spanish) Susaníbar Napurí LF, Simón Rodríguez C, López Martín L, Monzó Gardinier J, Cabello Benavente R, González Enguita C. https://www.aeurologia.com/EN/Y2011/V64/I1/62. Arch Esp Urol. 2011;64:62–66. - PubMed
Publication types
LinkOut - more resources
Full Text Sources