Assessment of Screening for Adverse Childhood Experiences and Receipt of Behavioral Health Services Among Children and Adolescents
- PMID: 36534401
- PMCID: PMC9857176
- DOI: 10.1001/jamanetworkopen.2022.47421
Assessment of Screening for Adverse Childhood Experiences and Receipt of Behavioral Health Services Among Children and Adolescents
Abstract
Importance: Screening for adverse childhood experiences (ACEs) in primary care settings has been increasing as a response to the overwhelming and consistent evidence of the deleterious associations between ACEs and later physical and mental health. However, there is little empirical guidance on the appropriate implementation of ACEs screening in pediatric primary care.
Objective: To test the use of a pilot intervention for ACEs screening and referral on the receipt of behavioral health care for children and adolescents within a large integrated health care delivery system.
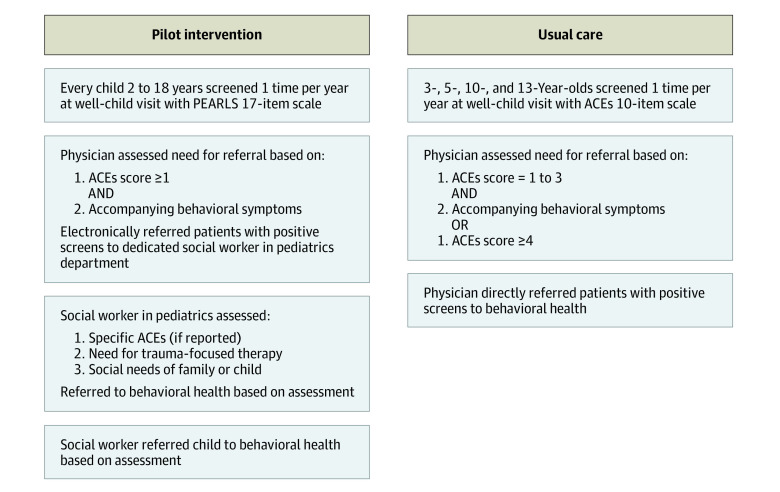
Design, setting, and participants: A retrospective cohort study was conducted in a large integrated health care system serving Southern California. Child and adolescent members of the target health care system younger than 18 years between July 1, 2018, and November 30, 2021, who received a positive screening for ACEs at the pilot clinic were included. This pilot clinic implemented an intervention that included additional screening questions and incorporated social workers into the process of evaluation and referral for behavioral health needs following ACEs screening.
Exposures: ACEs screening.
Main outcomes and measures: Visit to a behavioral health care service within 90 days of a positive ACEs screen determined as a score of 1 or higher and behavioral symptoms.
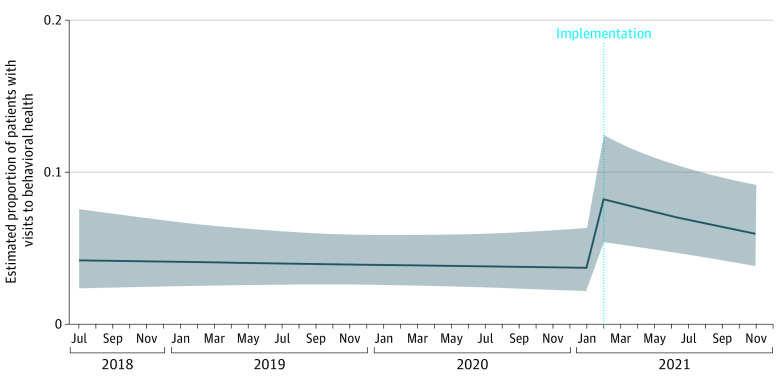
Results: The cohort consisted of 4030 children (mean [SD] age, 9.94 [4.55] years) with positive ACEs screening, 48% adolescents (11-17.99 years), approximately equal gender (51% females), 73% Hispanic, and 33% with Medicaid insurance. After the intervention, children were more likely to have a behavioral health services visit within 90 days of the screening than before the intervention (from 4.33% to 32.48%; incidence rate ratio, 7.50; 95% CI, 1.55-36.2).
Conclusions and relevance: In this cohort study, the implementation of a new ACEs screening and referral process was associated with increased receipt of behavioral health services among children with a positive ACEs screening. This could be useful strategy for other health care systems responding to state and local mandates to screen and provide care for children with ACEs.
Conflict of interest statement
Figures