

Percutaneous thrombectomy in patients with intermediate- and high-risk pulmonary embolism and contraindications to thrombolytics: a systematic review and meta-analysis
- PMID: 36536090
- PMCID: PMC9762655
- DOI: 10.1007/s11239-022-02750-1
Percutaneous thrombectomy in patients with intermediate- and high-risk pulmonary embolism and contraindications to thrombolytics: a systematic review and meta-analysis
Abstract
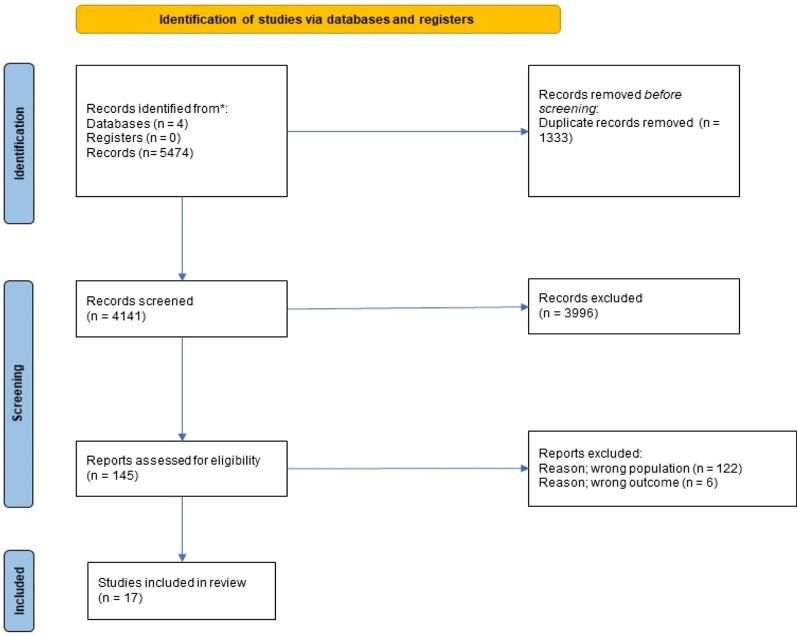
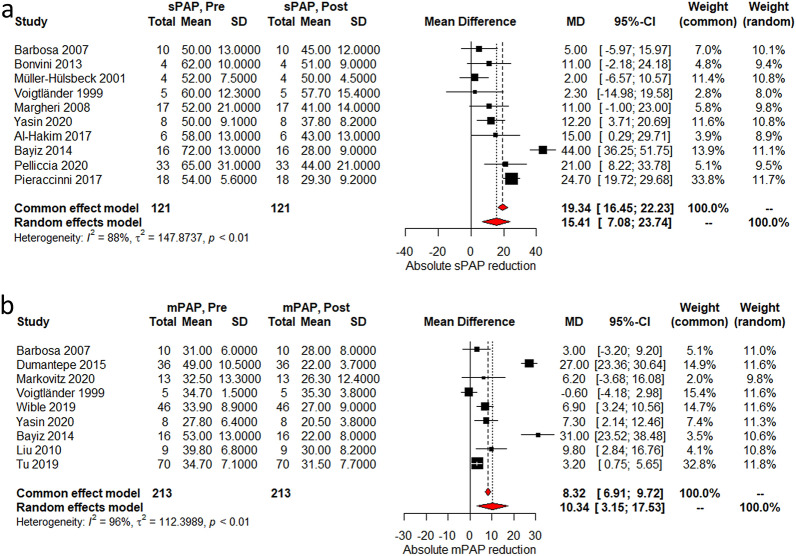
Catheter-directed interventions have slowly been gaining ground in the treatment of pulmonary embolism (PE), especially in patients with increased risk of bleeding. The goal of this study is to summarize the evidence for the efficacy and safety of percutaneous thrombectomy (PT) in patients with contraindications to systemic and local thrombolysis. We performed a systematic review and meta-analysis using MEDLINE, Cochrane, Scopus and the Web of Science databases for studies from inception to March 2022. We included patients with intermediate- and high-risk PE with contraindications to thrombolysis; patients who received systematic or local thrombolysis were excluded. Primary endpoint was in-hospital and 30-day mortality, with secondary outcomes based on hemodynamic and radiographic changes. Major bleeding events were assessed as a safety endpoint. Seventeen studies enrolled 455 patients, with a mean age of 58.6 years and encompassing 50.4% females. In-hospital and 30-day mortality rates were 4% (95% CI 3-6%) and 5% (95% CI 3-9%) for all-comers, respectively. We found a post-procedural reduction in systolic and mean pulmonary arterial pressures by 15.4 mmHg (95% CI 7-23.7) and 10.3 mmHg (95% CI 3.1-17.5) respectively. The RV/LV ratio and Miller Index were reduced by 0.42 (95% CI 0.38-46) and 7.8 (95% CI 5.2-10.5). Major bleeding events occurred in 4% (95% CI 3-6%). This is the first meta-analysis to report pooled outcomes on PT in intermediate- and high-risk PE patients without the use of systemic or local thrombolytics. The overall mortality rate is comparable to other contemporary treatments, and is an important modality particularly in those with contraindications for adjunctive thrombolytic therapy. Further studies are needed to understand the interplay of anticoagulation with PT and catheter-directed thrombolysis.
Keywords: Bleeding; Hemodynamics; Mortality; Percutaneous thrombectomy; Pulmonary embolism.
© 2022. The Author(s), under exclusive licence to Springer Science+Business Media, LLC, part of Springer Nature.
Conflict of interest statement
Dr. Shishehbor is a consultant for Abbott Vascular, Medtronic, Terumo, Philips, and Boston Scientific. Dr. Li is on the advisory board for Boston Scientific, Inari Medical, and Medtronic; she receives research funding from Abbott Vascular and Inari Medical. The rest of the authors have no conflicts of interest to disclose.
Figures





References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
