

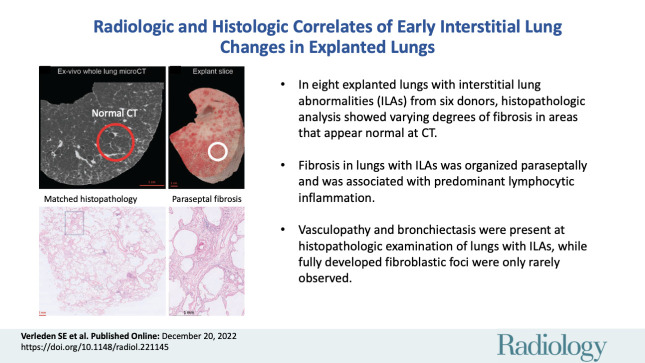
Radiologic and Histologic Correlates of Early Interstitial Lung Changes in Explanted Lungs
- PMID: 36537894
- PMCID: PMC7614383
- DOI: 10.1148/radiol.221145
Radiologic and Histologic Correlates of Early Interstitial Lung Changes in Explanted Lungs
Abstract
Background Interstitial lung abnormalities (ILAs) reflect imaging features on lung CT scans that are compatible with (early) interstitial lung disease. Despite accumulating evidence regarding the incidence, risk factors, and prognosis of ILAs, the histopathologic correlates of ILAs remain elusive. Purpose To determine the correlation between radiologic and histopathologic findings in CT-defined ILAs in human lung explants. Materials and Methods Explanted lungs or lobes from participants with radiologically documented ILAs were prospectively collected from 2010 to 2021. These specimens were air-inflated, frozen, and scanned with CT and micro-CT (spatial resolution of 0.7 mm and 90 μm, respectively). Subsequently, the lungs were cut and sampled with core biopsies. At least five samples per lung underwent micro-CT and subsequent histopathologic assessment with semiquantitative remodeling scorings. Based on area-specific radiologic scoring, the association between radiologic and histopathologic findings was assessed. Results Eight lung explants from six donors (median age at explantation, 71 years [range, 60-83 years]; four men) were included (unused donor lungs, n = 4; pre-emptive lobectomy for oncologic indications, n = 2). Ex vivo CT demonstrated ground-glass opacification, reticulation, and bronchiectasis. Micro-CT and histopathologic examination demonstrated that lung abnormalities were frequently paraseptal and associated with fibrosis and lymphocytic inflammation. The histopathologic results showed varying degrees of fibrosis in areas that appeared normal on CT scans. Regions of reticulation on CT scans generally had greater fibrosis at histopathologic analysis. Vasculopathy and bronchiectasis were also often present at histopathologic examination of lungs with ILAs. Fully developed fibroblastic foci were rarely observed. Conclusion This study demonstrated direct histologic correlates of CT-defined interstitial lung abnormalities. © RSNA, 2022 Supplemental material is available for this article. See also the editorial by Jeudy in this issue.
Conflict of interest statement
Figures
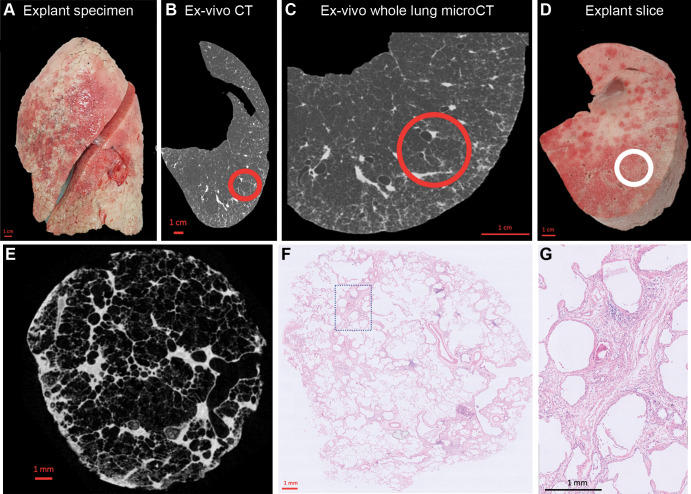
![Illustrative examples of sampled lung areas with ex vivo CT, micro-CT,
and histologic staining. (A) Axial noncontrast ex vivo CT scan shows highly
abnormal (25% healthy, 55% reticulation, 20% ground-glass opacification)
lung findings. (B–E) Micro-CT scan (B) and histopathologic images
(hematoxylin-eosin [C, D] and trichrome [E] staining; magnification,
×5 for C and E, ×20 for D) of the area highlighted with the
circle in A show paraseptal and interstitial fibrotic changes. (F) Axial
noncontrast ex vivo CT scan shows lung considered healthy (80%), with mild
ground-glass opacification (15%) and limited reticulation (5%). (G–J)
Micro-CT scan (G) and histopathologic images (hematoxylin-eosin [H, I] and
trichrome [J] staining; magnification, ×5 for H and J, ×20 for
I) of the matched location (circle in F) show paraseptal and interstitial
fibrosis. Awy = airway, BV = blood vessel.](https://cdn.ncbi.nlm.nih.gov/pmc/blobs/d2d5/10068885/bbfa56cd6dd6/radiol.221145.fig3.jpg)
Comment in
-
Interstitial Lung Abnormalities: The More We Learn, the Less We Know.Radiology. 2023 Apr;307(1):e222996. doi: 10.1148/radiol.222996. Epub 2022 Dec 20. Radiology. 2023. PMID: 36537900 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
