

Radiographic Cortical Thickness Index Predicts Fragility Fracture in Gaucher Disease
- PMID: 36537898
- PMCID: PMC7614382
- DOI: 10.1148/radiol.212779
Radiographic Cortical Thickness Index Predicts Fragility Fracture in Gaucher Disease
Abstract
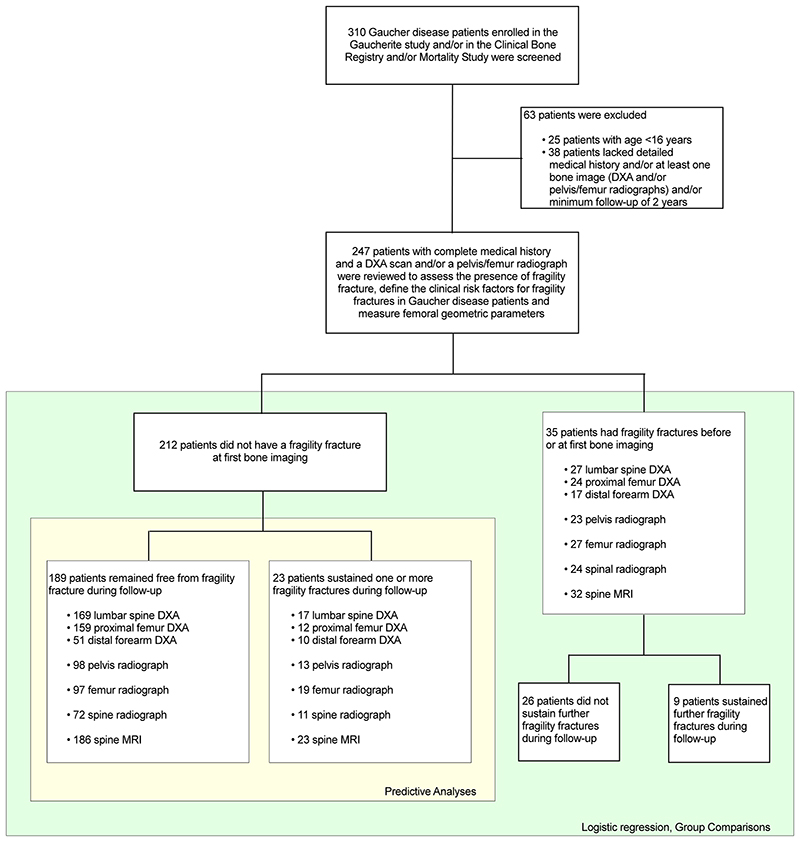
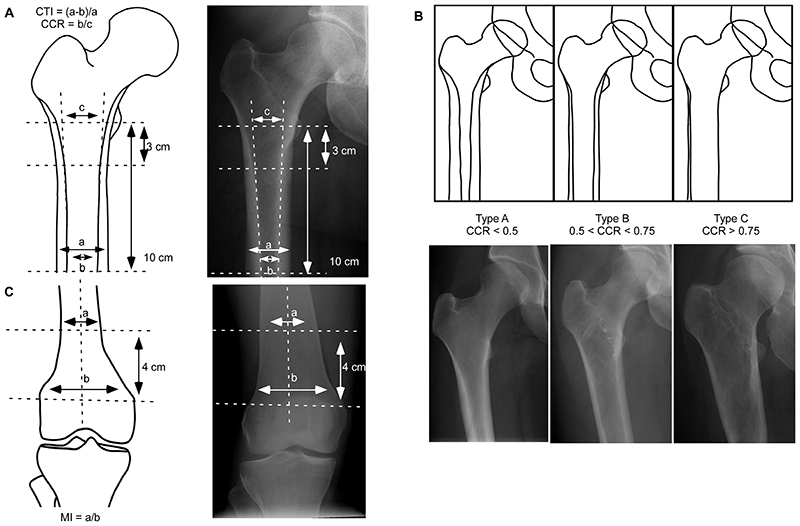
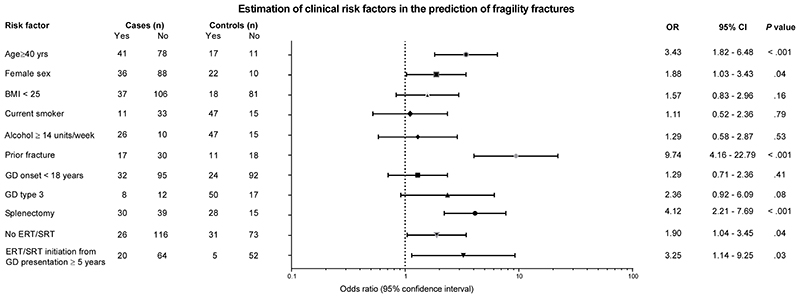
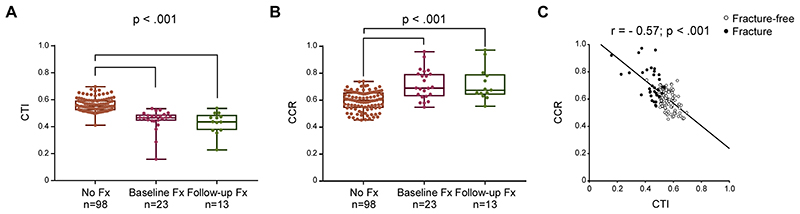
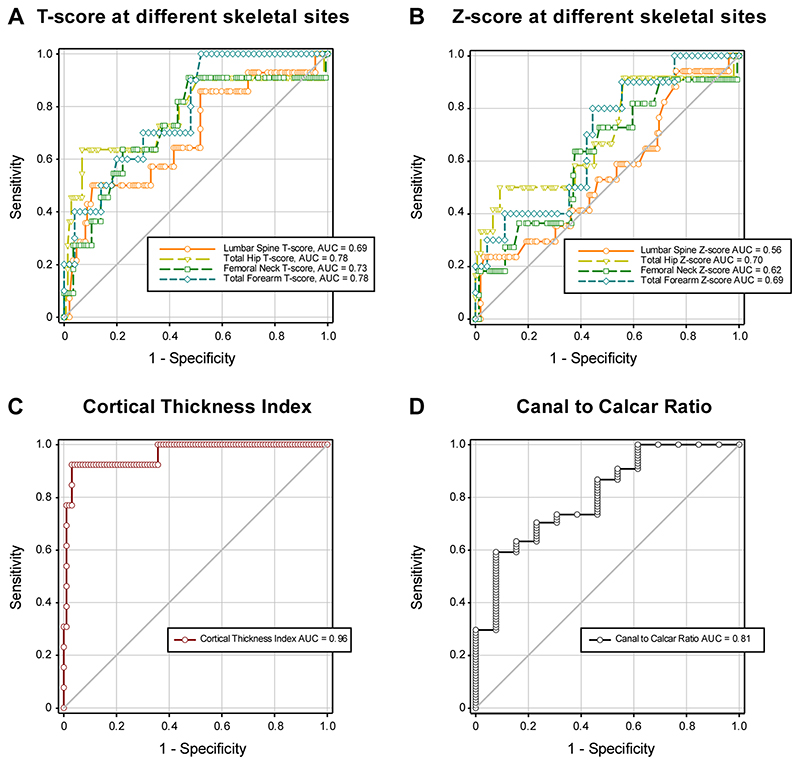
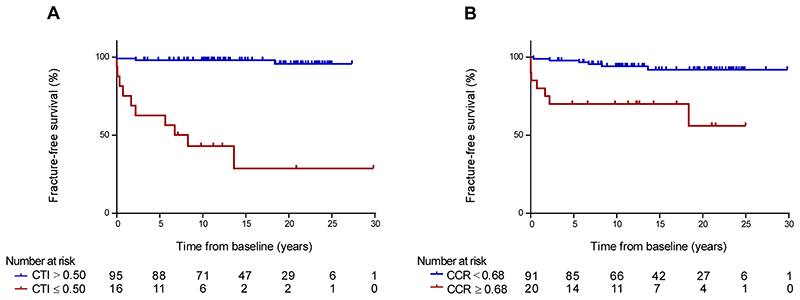
Background Patients with Gaucher disease (GD) have a high risk of fragility fractures. Routine evaluation of bone involvement in these patients includes radiography and repeated dual-energy x-ray absorptiometry (DXA). However, osteonecrosis and bone fracture may affect the accuracy of DXA. Purpose To assess the utility of DXA and radiographic femoral cortical thickness measurements as predictors of fragility fracture in patients with GD with long-term follow-up (up to 30 years). Materials and Methods Patients with GD age 16 years and older with a detailed medical history, at least one bone image (DXA and/or radiographs), and minimum 2 years follow-up were retrospectively identified using three merged UK-based registries (Gaucherite study, enrollment 2015-2017; Clinical Bone Registry, enrollment 2003-2006; and Mortality Registry, enrollment 1993-2019). Cortical thickness index (CTI) and canal-to-calcar ratio (CCR) were measured by two independent observers, and inter- and intraobserver reliability was calculated. The fracture-predictive value of DXA, CTI, CCR, and cutoff values were calculated using receiver operating characteristic curves. Statistical differences were assessed using univariable and multivariable analysis. Results Bone imaging in 247 patients (123 men, 124 women; baseline median age, 39 years; IQR, 27-50 years) was reviewed. The median follow-up period was 11 years (IQR, 7-19 years; range, 2-30 years). Thirty-five patients had fractures before or at first bone imaging, 23 patients had fractures after first bone imaging, and 189 patients remained fracture-free. Inter- and intraobserver reproducibility for CTI/CCR measurements was substantial (range, 0.96-0.98). In the 212 patients with no baseline fracture, CTI (cutoff, ≤0.50) predicted future fractures with higher sensitivity and specificity (area under the receiver operating characteristic curve [AUC], 0.96; 95% CI: 0.84, 0.99; sensitivity, 92%; specificity, 96%) than DXA T-score at total hip (AUC, 0.78; 95% CI: 0.51, 0.91; sensitivity, 64%; specificity, 93%), femoral neck (AUC, 0.73; 95% CI: 0.50, 0.86; sensitivity, 64%; specificity, 73%), lumbar spine (AUC, 0.69; 95% CI: 0.49, 0.82; sensitivity, 57%; specificity, 63%), and forearm (AUC, 0.78; 95% CI: 0.59, 0.89; sensitivity, 70%; specificity, 70%). Conclusion Radiographic cortical thickness index of 0.50 or less was a reliable independent predictor of fracture risk in Gaucher disease. Clinical trial registration no. NCT03240653 © RSNA, 2022 Supplemental material is available for this article.
Conflict of interest statement
SD reports speaker fees from Takeda and travel support from Sanofi Genzyme and Takeda outside of the submitted work; and has been recently employed by Chiesi (after the submission of this manuscript). PD reports research grant support from Sanofi Genzyme and Takeda; speaker fee from Sanofi Genzyme and Takeda outside of the submitted work; and is a member of European Board of the International Collaborative Gaucher Group Gaucher Registry (ICGG), which is sponsored by Sanofi Genzyme, and of the Gaucher Outcome Survey Board Member, which is sponsored by Takeda. TMC reports research grant support from Sanofi and Takeda; consulting and speaker fees from Avrobio, Sanofi Genzyme, and Takeda; travel support from Sanofi Genzyme; and advisory board fees from Sanofi Genzyme outside of the submitted work. UR reports research grant support from Amicus, Intrabio, and Takeda; consulting and speaker fees, and travel support from Amicus, Sanofi Genzyme, and Takeda outside of the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Multifactorial Impact on Bone Fragility in Gaucher Disease.Radiology. 2023 Jun;307(5):e230140. doi: 10.1148/radiol.230140. Radiology. 2023. PMID: 37367449 No abstract available.
References
-
- Roh J, Subramanian S, Weinreb NJ, Kartha RV. Gaucher disease - more than just a rare lipid storage disease. J Mol Med (Berl) 2022;100:499–518. - PubMed
-
- Wenstrup RJ, Kacena KA, Kaplan P, et al. Effect of enzyme replacement therapy with imiglucerase on BMD in type 1 Gaucher disease. J Bone Miner Res. 2007;22:119–126. - PubMed
-
- Khan A, Hangartner T, Weinreb NJ, Taylor JS, Mistry PK. Risk factors for fractures and avascular osteonecrosis in type 1 Gaucher disease: a study from the International Collaborative Gaucher Group (ICGG) Gaucher Registry. J Bone Miner Res. 2012;27:1839–1848. - PubMed
-
- Leslie WD, Tsang JF, Caetano PA, Lix LM. Effectiveness of bone density measurement for predicting osteoporotic fractures in clinical practice. J Clin Endocrinol Metab. 2007;92:77–81. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
