

Evidence-Based High-Loading Tendon Exercise for 12 Weeks Leads to Increased Tendon Stiffness and Cross-Sectional Area in Achilles Tendinopathy: A Controlled Clinical Trial
- PMID: 36538166
- PMCID: PMC9768072
- DOI: 10.1186/s40798-022-00545-5
Evidence-Based High-Loading Tendon Exercise for 12 Weeks Leads to Increased Tendon Stiffness and Cross-Sectional Area in Achilles Tendinopathy: A Controlled Clinical Trial
Abstract
Background: Assuming that the mechanisms inducing adaptation in healthy tendons yield similar responses in tendinopathic tendons, we hypothesized that a high-loading exercise protocol that increases tendon stiffness and cross-sectional area in male healthy Achilles tendons may also induce comparable beneficial adaptations in male tendinopathic Achilles tendons in addition to improving pain and function.
Objectives: We investigated the effectiveness of high-loading exercise in Achilles tendinopathy in terms of inducing mechanical (tendon stiffness, maximum strain), material (Young's modulus), morphological (tendon cross-sectional area (CSA)), maximum voluntary isometric plantar flexor strength (MVC) as well as clinical adaptations (Victorian Institute of Sports Assessment-Achilles (VISA-A) score and pain (numerical rating scale (NRS))) as the primary outcomes. As secondary outcomes, drop (DJ) and counter-movement jump (CMJ) height and intratendinous vascularity were assessed.
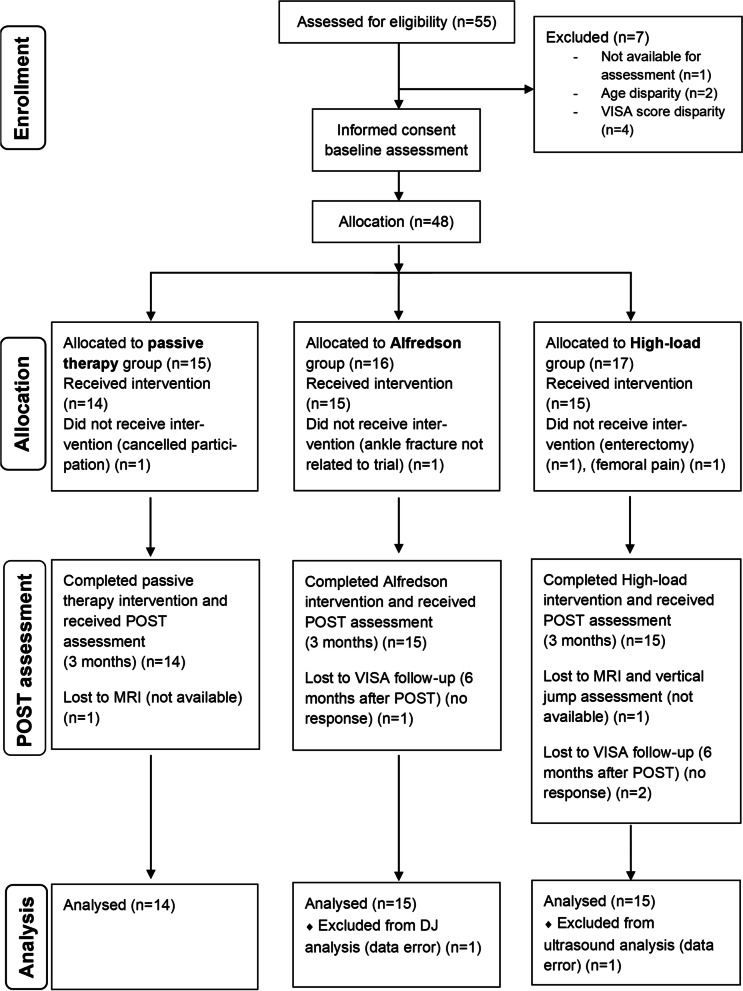
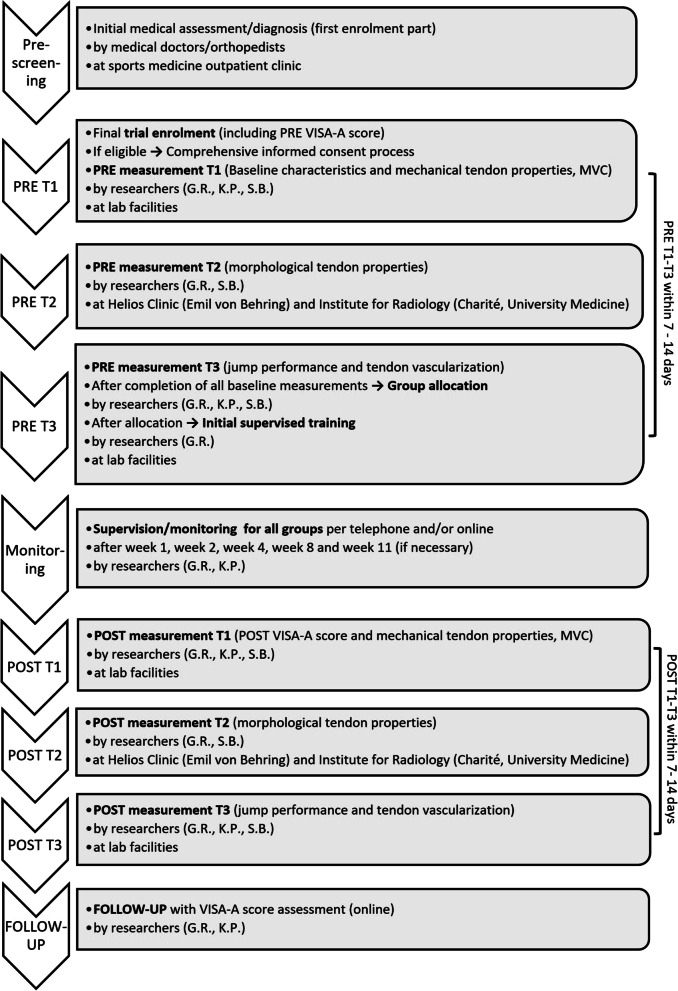
Methods: We conducted a controlled clinical trial with a 3-month intervention phase. Eligibility criteria were assessed by researchers and medical doctors. Inclusion criteria were male sex, aged between 20 and 55 years, chronic Achilles tendinopathy confirmed by a medical doctor via ultrasound-assisted assessment, and a severity level of less than 80 points on the VISA-A score. Thirty-nine patients were assigned by sequential allocation to one of three parallel arms: a high-loading intervention (training at ~ 90% of the MVC) (n = 15), eccentric exercise (according to the Alfredson protocol) as the standard therapy (n = 15) and passive therapy (n = 14). Parameters were assessed pre- and-post-intervention. Data analysis was blinded.
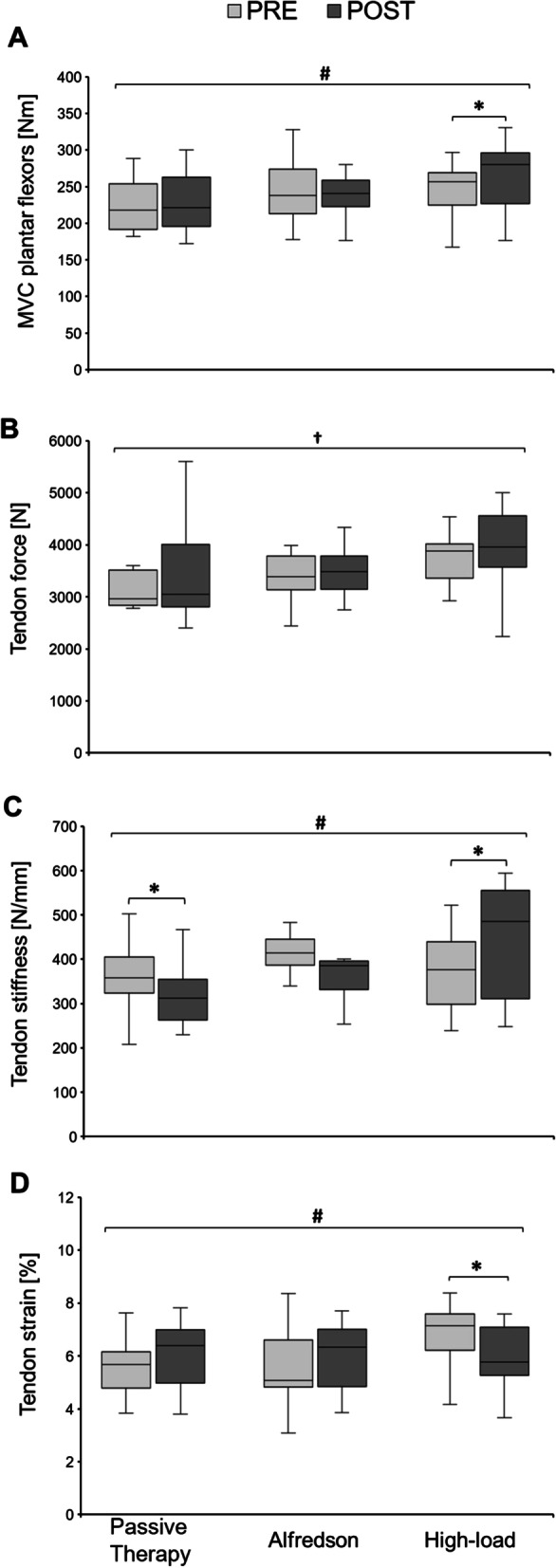
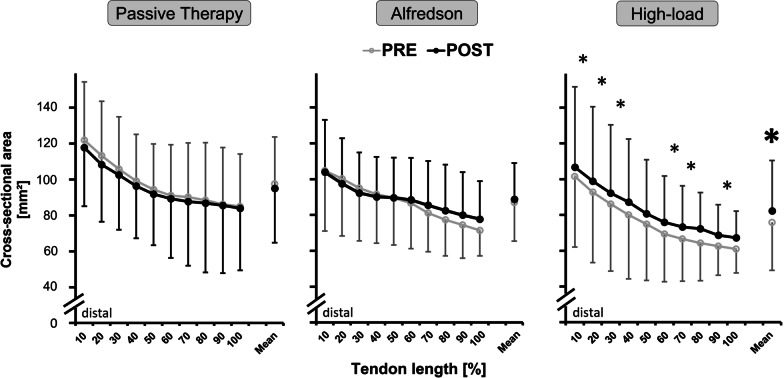
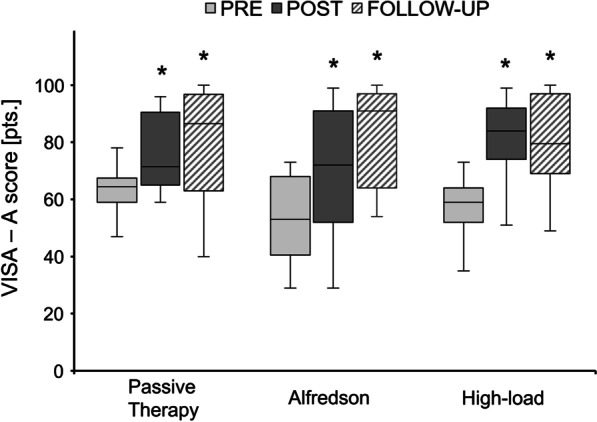
Results: Primary outcomes: Plantar flexor MVC, tendon stiffness, mean CSA and maximum tendon strain improved only in the high-loading intervention group by 7.2 ± 9.9% (p = 0.045), 20.1 ± 20.5% (p = 0.049), 8.98 ± 5.8% (p < 0.001) and -12.4 ± 10.3% (p = 0.001), respectively. Stiffness decreased in the passive therapy group (-7.7 ± 21.2%; p = 0.042). There was no change in Young's modulus in either group (p > 0.05). The VISA-A score increased in all groups on average by 19.8 ± 15.3 points (p < 0.001), while pain (NRS) dropped by -0.55 ± 0.9 points (p < 0.001).
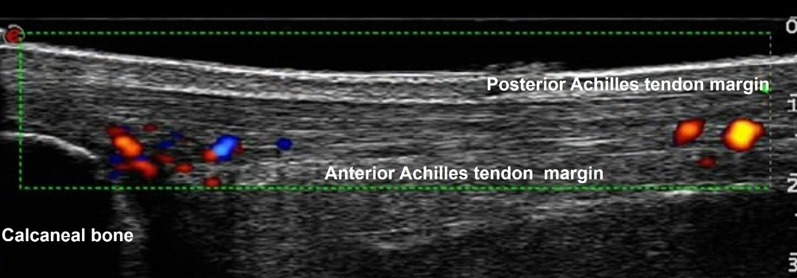
Secondary outcomes: CMJ height decreased for all groups (-0.63 ± 4.07 cm; p = 0.005). There was no change in DJ height and vascularity (p > 0.05) in either group.
Conclusion: Despite an overall clinical improvement, it was exclusively the high-loading intervention that induced significant mechanical and morphological adaptations of the plantar flexor muscle-tendon unit. This might contribute to protecting the tendon from strain-induced injury. Thus, we recommend the high-loading intervention as an effective (alternative) therapeutic protocol in Achilles tendinopathy rehabilitation management in males.
Clinical trials registration number: NCT02732782.
Keywords: Achilles tendinopathy; Controlled clinical trial; Eccentric training; High-loading exercise; Musculoskeletal rehabilitation; Physiotherapy; Tendon adaptation; Tendon rehabilitation; Training therapy.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Legerlotz K. Rehabilitation of tendopathies in human athletes. Comp Exerc Physiol. 2013;9:153–160. doi: 10.3920/CEP13030. - DOI
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
