

Management of Acute Stress Reactions in the Military: A Stepped Care Approach
- PMID: 36538195
- PMCID: PMC9780143
- DOI: 10.1007/s11920-022-01388-3
Management of Acute Stress Reactions in the Military: A Stepped Care Approach
Abstract
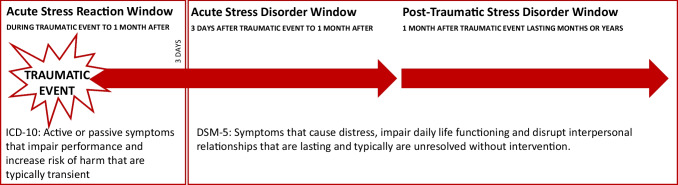
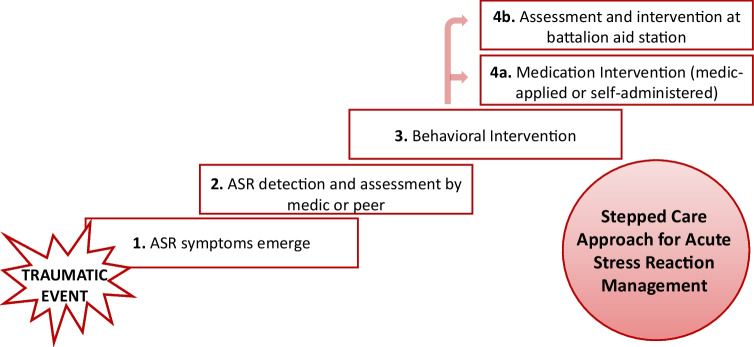
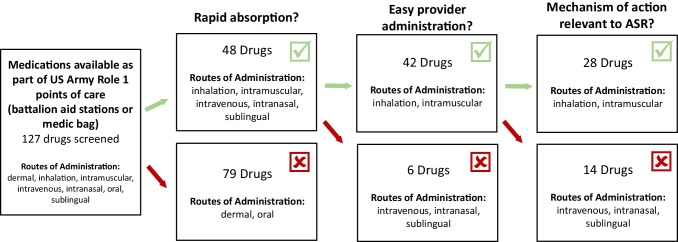
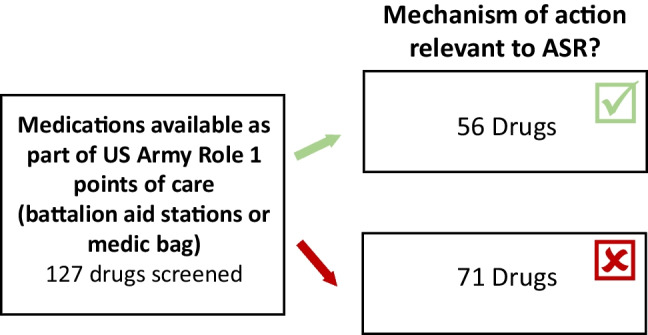
Purpose of the review: This review highlights knowledge gaps surrounding the development and use of interventions for Acute Stress Reactions (ASRs). First, we propose that a stepped care approach to intervention for ASR be developed and utilized in military operational environments. A stepped care approach would include detection and assessment, followed by behavioral intervention, and then medication intervention for ASRs. Second, we discuss potential strategies that can be taken for the development of safe and effective ASR medications.
Recent findings: ASRs commonly occur in operational environments, particularly in military populations. ASRs impact the safety and performance of individual service members and teams, but there are currently limited options for intervention. Efforts to improve ASR detection and assessment, and development and delivery of ASR interventions for implementation in operational environments, will be critical to maintaining the safety and performance of service members.
Keywords: Acute traumatic stress; Assessment; Intervention; Medication; Pharmacologic; iCOVER.
© 2022. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 2013:Vol. 5th Edition.
-
- World Health Organization, International statistical classification of diseases and related health problems (ICD-11). 2019;11th Edition.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
