

Effect of Pessary vs Surgery on Patient-Reported Improvement in Patients With Symptomatic Pelvic Organ Prolapse: A Randomized Clinical Trial
- PMID: 36538310
- PMCID: PMC9857016
- DOI: 10.1001/jama.2022.22385
Effect of Pessary vs Surgery on Patient-Reported Improvement in Patients With Symptomatic Pelvic Organ Prolapse: A Randomized Clinical Trial
Abstract
Importance: Pelvic organ prolapse is a prevalent condition among women that negatively affects their quality of life. With increasing life expectancy, the global need for cost-effective care for women with pelvic organ prolapse will continue to increase.
Objective: To investigate whether treatment with a pessary is noninferior to surgery among patients with symptomatic pelvic organ prolapse.
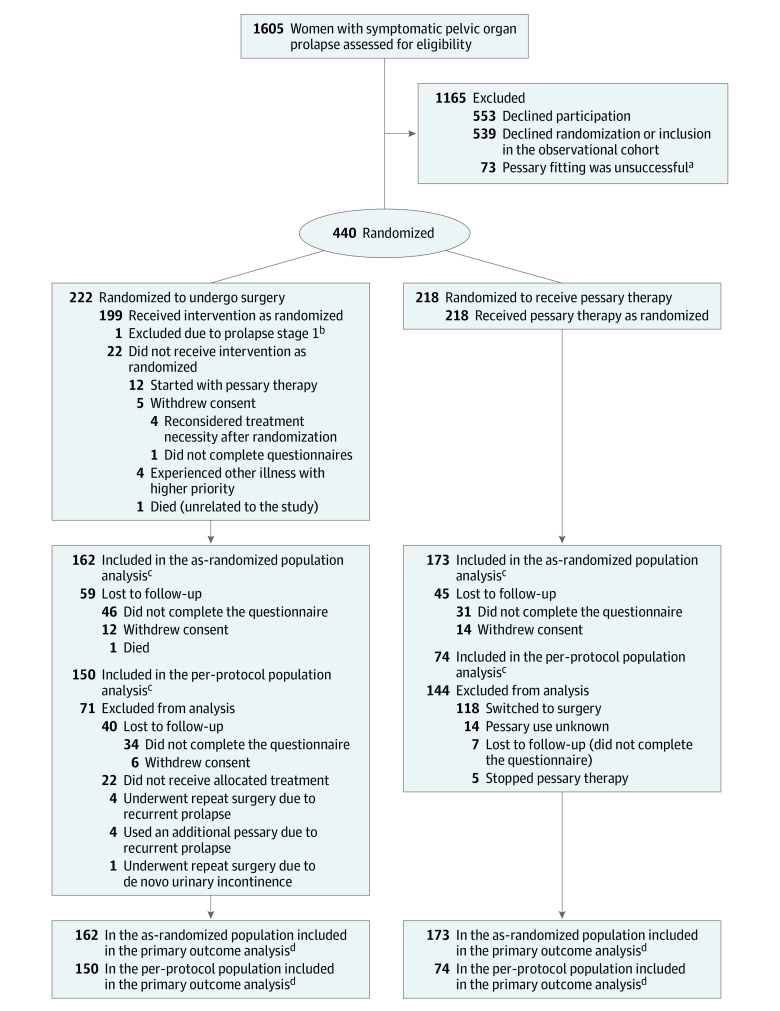
Design, setting, and participants: The PEOPLE project was a noninferiority randomized clinical trial conducted in 21 participating hospitals in the Netherlands. A total of 1605 women with symptomatic stage 2 or greater pelvic organ prolapse were requested to participate between March 2015 through November 2019; 440 gave informed consent. Final 24-month follow-up ended at June 30, 2022.
Interventions: Two hundred eighteen participants were randomized to receive pessary treatment and 222 to surgery.
Main outcomes and measures: The primary outcome was subjective patient-reported improvement at 24 months, measured with the Patient Global Impression of Improvement scale, a 7-point Likert scale ranging from very much better to very much worse. This scale was dichotomized as successful, defined as much better or very much better, vs nonsuccessful treatment. The noninferiority margin was set at 10 percentage points risk difference. Data of crossover between therapies and adverse events were captured.
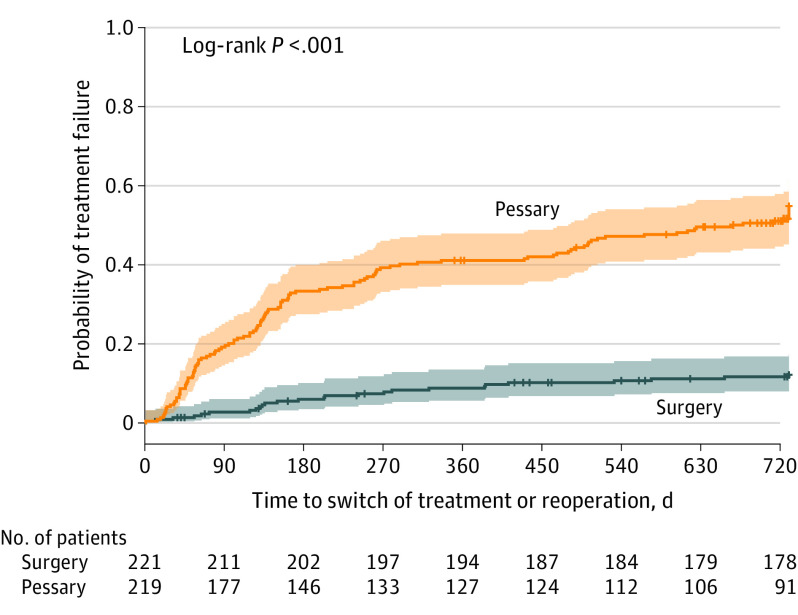
Results: Among 440 patients who were randomized (mean [SD] age, 64.7 [9.29] years), 173 (79.3%) in the pessary group and 162 (73.3%) in the surgery group completed the trial at 24 months. In the population, analyzed as randomized, subjective improvement was reported by 132 of 173 (76.3%) in the pessary group vs 132 of 162 (81.5%) in the surgery group (risk difference, -6.1% [1-sided 95% CI, -12.7 to ∞]; P value for noninferiority, .16). The per-protocol analysis showed a similar result for subjective improvement with 52 of 74 (70.3%) in the pessary group vs 125 of 150 (83.3%) in the surgery group (risk difference, -13.1% [1-sided 95% CI, -23.0 to ∞]; P value for noninferiority, .69). Crossover from pessary to surgery occurred among 118 of 218 (54.1%) participants. The most common adverse event among pessary users was discomfort (42.7%) vs urinary tract infection (9%) following surgery.
Conclusions and relevance: Among patients with symptomatic pelvic organ prolapse, an initial strategy of pessary therapy, compared with surgery, did not meet criteria for noninferiority with regard to patient-reported improvement at 24 months. Interpretation is limited by loss to follow-up and the large amount of participant crossover from pessary therapy to surgery.
Trial registration: Netherlands Trial Register Identifier: NTR4883.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
