

Comparative efficacy of tezepelumab to mepolizumab, benralizumab, and dupilumab in eosinophilic asthma: A Bayesian network meta-analysis
- PMID: 36538979
- PMCID: PMC9992307
- DOI: 10.1016/j.jaci.2022.11.021
Comparative efficacy of tezepelumab to mepolizumab, benralizumab, and dupilumab in eosinophilic asthma: A Bayesian network meta-analysis
Abstract
Background: It is unclear how the efficacy of tezepelumab, approved for the treatment of type 2 high and low asthma, compares to the efficacy of other biologics for type 2-high asthma.
Objectives: We sought to conduct an indirect comparison of tezepelumab to dupilumab, benralizumab, and mepolizumab in the treatment of eosinophilic asthma.
Methods: The investigators conducted a systematic review and Bayesian network meta-analyses. They identified randomized controlled trials indexed in PubMed, Embase, or Cochrane Central Register of Controlled Trials (CENTRAL) between January 1, 2000, and August 12, 2022. Outcomes included exacerbation rates, prebronchodilator FEV1, and the Asthma Control Questionnaire.
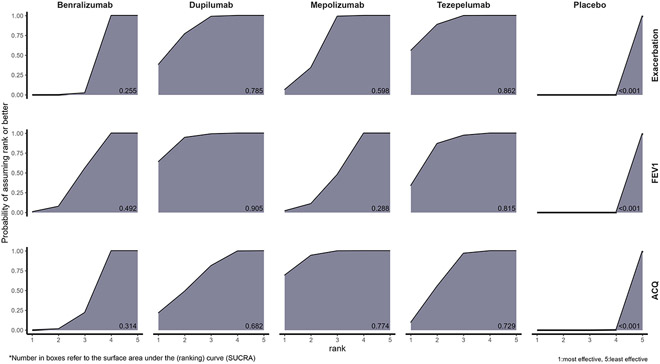
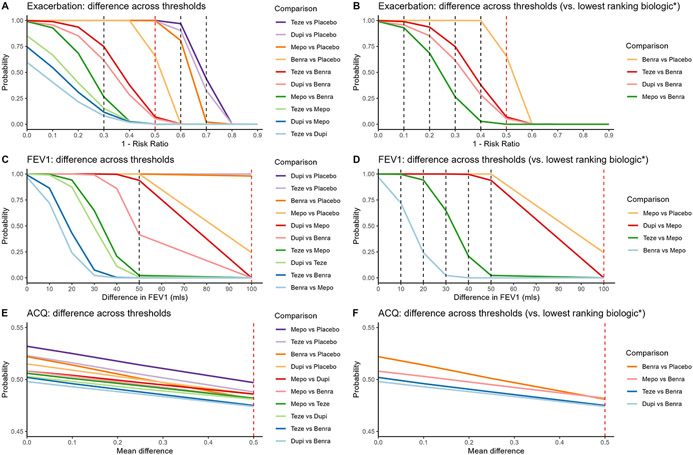
Results: Ten randomized controlled trials (n = 9201) met eligibility. Tezepelumab (relative risk: 0.63; 95% credible interval [CI]: 0.46-0.86) was associated with significantly lower exacerbation rates than benralizumab and larger improvements in FEV1 compared to mepolizumab (mean difference [MD]: 66; 95% CI: -33 to 170) and benralizumab (MD: 62; 95% CI: -22 to 150), though the 95% CI crossed the null value of 0. Mepolizumab improved the Asthma Control Questionnaire score the most, but this improvement was not significantly different from that of tezepelumab (tezepelumab vs mepolizumab; MD: 0.14; 95% CI: -0.10 to 0.38). For efficacy by clinically important thresholds, tezepelumab, mepolizumab, and dupilumab achieved a >99% probability of reducing exacerbation rates by ≥50% compared to placebo, but benralizumab had only a 66% probability of doing so. Tezepelumab and dupilumab had a probability of 1.00 of improving prebronchodilator FEV1 by ≥100 mL above placebo. Compared to mepolizumab, dupilumab had >90% chance for improving FEV1 by ≥50 mL, but none of the differences between biologics exceeded 100 mL.
Conclusions: In individuals with eosinophilic asthma, tezepelumab and dupilumab were associated with greater improvements (although below clinical thresholds) in exacerbation rates and lung function than benralizumab or mepolizumab.
Keywords: Asthma; Bayesian; benralizumab; comparative effectiveness; dupilumab; eosinophilic; mAb; mepolizumab; network meta-analysis; tezepelumab.
Copyright © 2022 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosures:
Dr. Alexander is past Chair and a current member of FDA’s Peripheral and Central Nervous System Advisory Committee; is a co-founding Principal and equity holder in Monument Analytics, a health care consultancy whose clients include the life sciences industry as well as plaintiffs in opioid litigation, for whom he has served as a paid expert witness; and is a past member of OptumRx’s National P&T Committee. This arrangement has been reviewed and approved by Johns Hopkins University in accordance with its conflict-of-interest policies. All other authors have no relevant conflicts of interest to disclose.
Figures

References
-
- Antonicelli L, Bucca C, Neri M, De Benedetto F, Sabbatani P, Bonifazi F, et al. Asthma severity and medical resource utilisation. Eur Respir J. 2004/06/05 ed. 2004. May;23(5):723–9. - PubMed
-
- Sullivan SD, Rasouliyan L, Russo PA, Kamath T, Chipps BE. Extent, patterns, and burden of uncontrolled disease in severe or difficult-to-treat asthma. Allergy. 2007/02/15 ed. 2007. Feb;62(2):126–33. - PubMed
-
- Chen S, Golam S, Myers J, Bly C, Smolen H, Xu X. Systematic literature review of the clinical, humanistic, and economic burden associated with asthma uncontrolled by GINA Steps 4 or 5 treatment. Curr Med Res Opin. 2018. Dec;34(12):2075–88. - PubMed
-
- US Food & Drug Administration. Novel Drug Approvals for 2015 [Internet]. 2015. [cited 2022 Sep 5]. Available from: https://www.fda.gov/drugs/new-drugs-fda-cders-new-molecular-entities-and...
-
- US Food & Drug Administration. Novel Drug Approvals for 2017 [Internet]. 2017. [cited 2022 Sep 5]. Available from: https://www.fda.gov/drugs/new-drugs-fda-cders-new-molecular-entities-and...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
