

Associations Between Polygenic Risk Score Loading, Psychosis Liability, and Clozapine Use Among Individuals With Schizophrenia
- PMID: 36542388
- PMCID: PMC9857760
- DOI: 10.1001/jamapsychiatry.2022.4234
Associations Between Polygenic Risk Score Loading, Psychosis Liability, and Clozapine Use Among Individuals With Schizophrenia
Abstract
Importance: Predictors consistently associated with psychosis liability and course of illness in schizophrenia (SCZ) spectrum disorders (SSD), including the need for clozapine treatment, are lacking. Longitudinally ascertained medication use may empower studies examining associations between polygenic risk scores (PRSs) and pharmacotherapy choices.
Objective: To examine associations between PRS-SCZ loading and groups with different liabilities to SSD (individuals with SSD taking clozapine, individuals with SSD taking other antipsychotics, their parents and siblings, and unrelated healthy controls) and between PRS-SCZ and the likelihood of receiving a prescription of clozapine relative to other antipsychotics.
Design, setting, and participants: This genetic association study was a multicenter, observational cohort study with 6 years of follow-up. Included were individuals diagnosed with SSD who were taking clozapine or other antipsychotics, their parents and siblings, and unrelated healthy controls. Data were collected from 2004 until 2021 and analyzed between October 2021 and September 2022.
Exposures: Polygenic risk scores for SCZ.
Main outcomes and measures: Multinomial logistic regression was used to examine possible differences between groups by computing risk ratios (RRs), ie, ratios of the probability of pertaining to a particular group divided by the probability of healthy control status. We also computed PRS-informed odd ratios (ORs) for clozapine use relative to other antipsychotics.
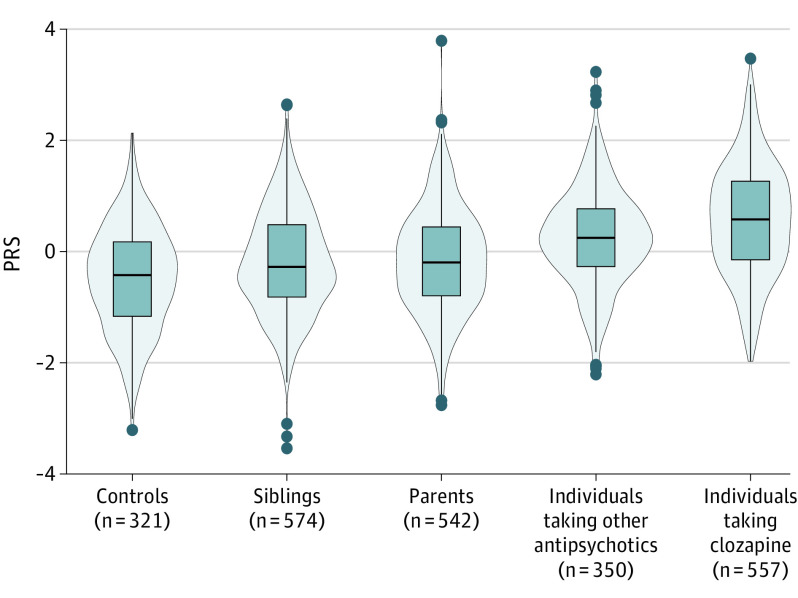
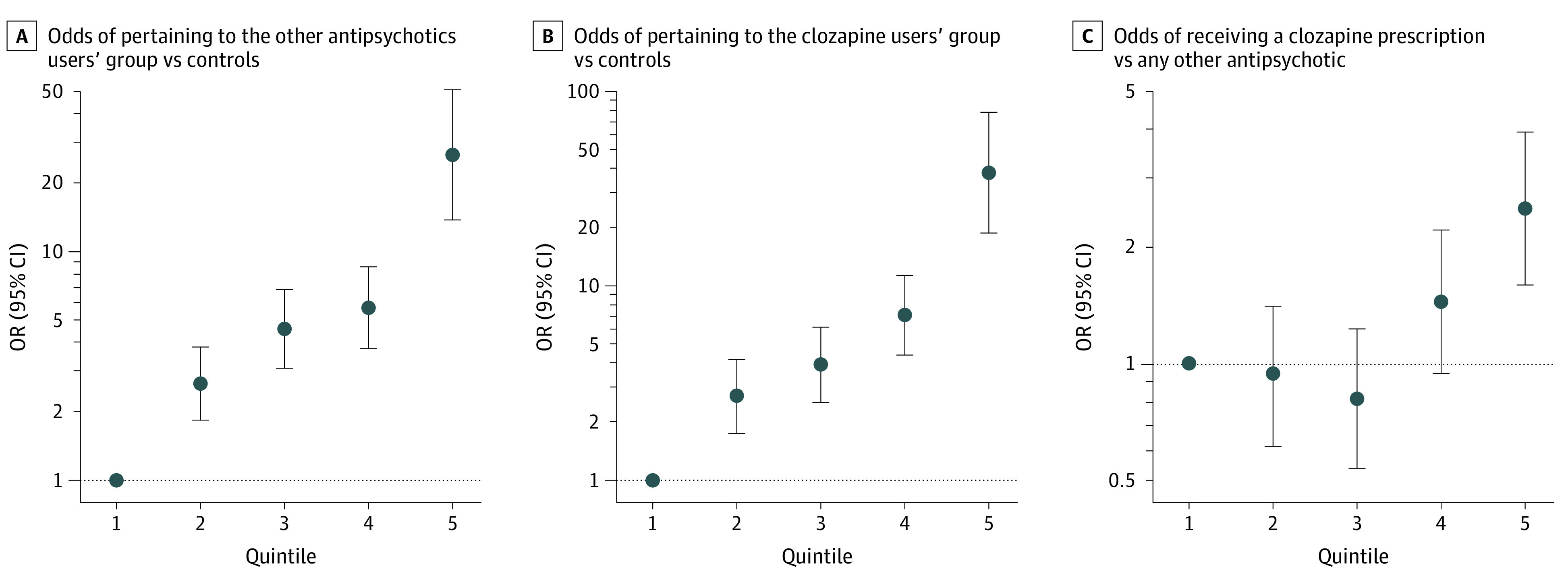
Results: Polygenic risk scores for SCZ were generated for 2344 participants (mean [SD] age, 36.95 years [14.38]; 994 female individuals [42.4%]) who remained after quality control screening (557 individuals with SSD taking clozapine, 350 individuals with SSD taking other antipsychotics during the 6-year follow-up, 542 parents and 574 siblings of individuals with SSD, and 321 unrelated healthy controls). All RRs were significantly different from 1; RRs were highest for individuals with SSD taking clozapine (RR, 3.24; 95% CI, 2.76-3.81; P = 2.47 × 10-46), followed by individuals with SSD taking other antipsychotics (RR, 2.30; 95% CI, 1.95-2.72; P = 3.77 × 10-22), parents (RR, 1.44; 95% CI, 1.25-1.68; P = 1.76 × 10-6), and siblings (RR, 1.40; 95% CI, 1.21-1.63; P = 8.22 × 10-6). Polygenic risk scores for SCZ were positively associated with clozapine vs other antipsychotic use (OR, 1.41; 95% CI, 1.22-1.63; P = 2.98 × 10-6), suggesting a higher likelihood of clozapine prescriptions among individuals with higher PRS-SCZ.
Conclusions and relevance: In this study, PRS-SCZ loading differed between groups of individuals with SSD, their relatives, and unrelated healthy controls, with patients taking clozapine at the far end of PRS-SCZ loading. Additionally, PRS-SCZ was associated with a higher likelihood of clozapine prescribing. Our findings may inform early intervention and prognostic studies of the value of using PRS-SCZ to personalize antipsychotic treatment.
Conflict of interest statement
Figures
References
-
- Trubetskoy V, Pardiñas AF, Qi T, et al. ; Indonesia Schizophrenia Consortium; PsychENCODE; Psychosis Endophenotypes International Consortium; SynGO Consortium; Schizophrenia Working Group of the Psychiatric Genomics Consortium . Mapping genomic loci implicates genes and synaptic biology in schizophrenia. Nature. 2022;604(7906):502-508. doi:10.1038/s41586-022-04434-5 - DOI - PMC - PubMed
-
- Ni G, Zeng J, Revez JA, et al. ; Schizophrenia Working Group of the Psychiatric Genomics Consortium; Major Depressive Disorder Working Group of the Psychiatric Genomics Consortium . A comparison of ten polygenic score methods for psychiatric disorders applied across multiple cohorts. Biol Psychiatry. 2021;90(9):611-620. doi:10.1016/j.biopsych.2021.04.018 - DOI - PMC - PubMed
-
- Amare AT, Schubert KO, Hou L, et al. ; Major Depressive Disorder Working Group of the Psychiatric Genomics Consortium . Association of polygenic score for major depression with response to lithium in patients with bipolar disorder. Mol Psychiatry. 2021;26(6):2457-2470. doi:10.1038/s41380-020-0689-5 - DOI - PubMed
-
- Coleman JRI, Gaspar HA, Bryois J, Breen G; Bipolar Disorder Working Group of the Psychiatric Genomics Consortium; Major Depressive Disorder Working Group of the Psychiatric Genomics Consortium . The genetics of the mood disorder spectrum: genome-wide association analyses of more than 185,000 cases and 439,000 controls. Biol Psychiatry. 2020;88(2):169-184. doi:10.1016/j.biopsych.2019.10.015 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
