

Zone 1 Endovascular Balloon Occlusion of the Aorta vs Resuscitative Thoracotomy for Patient Resuscitation After Severe Hemorrhagic Shock
- PMID: 36542395
- PMCID: PMC9856952
- DOI: 10.1001/jamasurg.2022.6393
Zone 1 Endovascular Balloon Occlusion of the Aorta vs Resuscitative Thoracotomy for Patient Resuscitation After Severe Hemorrhagic Shock
Abstract
Importance: Aortic occlusion (AO) is a lifesaving therapy for the treatment of severe traumatic hemorrhagic shock; however, there remains controversy whether AO should be accomplished via resuscitative thoracotomy (RT) or via endovascular balloon occlusion of the aorta (REBOA) in zone 1.
Objective: To compare outcomes of AO via RT vs REBOA zone 1.
Design, setting, and participants: This was a comparative effectiveness research study using a multicenter registry of postinjury AO from October 2013 to September 2021. AO via REBOA zone 1 (above celiac artery) was compared with RT performed in the emergency department of facilities experienced in both procedures and documented in the prospective multicenter Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery (AORTA) registry. Propensity score matching (PSM) with exact institution matching was used, in addition to subgroup multivariate analysis to control for confounders. The study setting included the ED, where AO via RT or REBOA was performed, and participants were adult trauma patients 16 years or older.
Exposures: AO via REBOA zone 1 vs RT.
Main outcomes and measures: The primary outcome was survival. Secondary outcomes were ventilation-free days (VFDs), intensive care unit (ICU)-free days, discharge Glasgow Coma Scale score, and Glasgow Outcome Score (GOS).
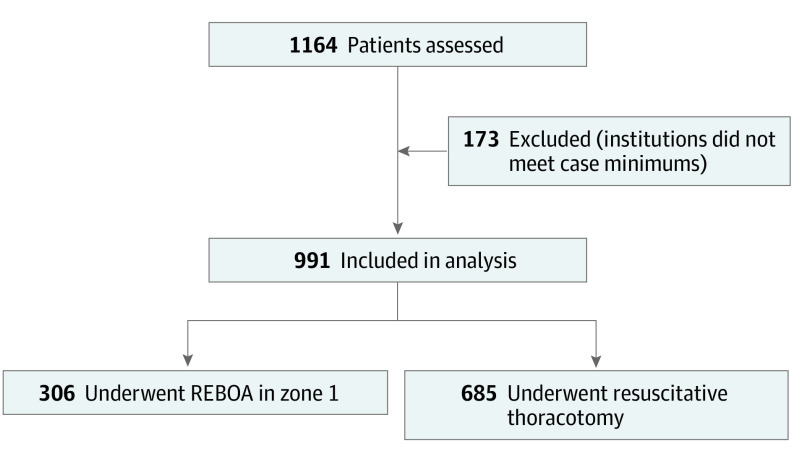
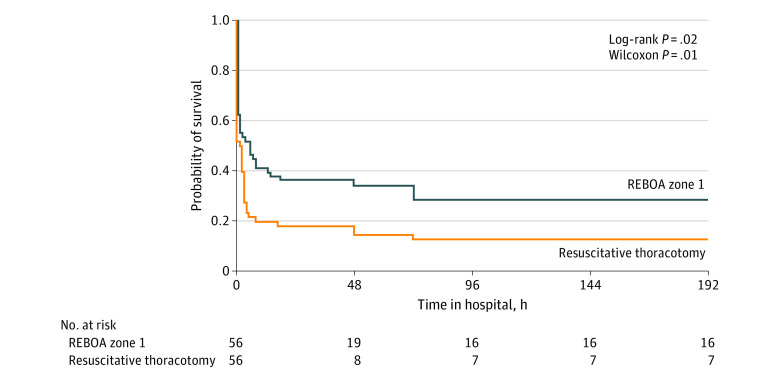
Results: A total of 991 patients (median [IQR] age, 32 [25-48] years; 808 male individuals [81.9%]) with a median (IQR) Injury Severity Score of 29 (18-50) were included. Of the total participants, 306 (30.9%) had AO via REBOA zone 1, and 685 (69.1%) had AO via RT. PSM selected 112 comparable patients (56 pairs). REBOA zone 1 was associated with a statistically significant lower mortality compared with RT (78.6% [44] vs 92.9% [52]; P = .03). There were no significant differences in VFD greater than 0 (REBOA, 18.5% [10] vs RT, 7.1% [4]; P = .07), ICU-free days greater than 0 (REBOA, 18.2% [10] vs RT, 7.1% [4]; P = .08), or discharge GOS of 5 or more (REBOA, 7.5% [4] vs RT, 3.6% [2]; P = .38). Multivariate analysis confirmed the survival benefit of REBOA zone 1 after adjustment for significant confounders (relative risk [RR], 1.25; 95% CI, 1.15-1.36). In all subgroup analyses (cardiopulmonary resuscitation on arrival, traumatic brain injury, chest injury, pelvic injury, blunt/penetrating mechanism, systolic blood pressure ≤60 mm Hg on AO initiation), REBOA zone 1 offered an either similar or superior survival.
Conclusions and relevance: Results of this comparative effectiveness research suggest that REBOA zone 1 provided better or similar survival than RT for patients requiring AO postinjury. These findings provide the ethically necessary equipoise between these therapeutic approaches to allow the planning of a randomized controlled trial to establish the safety and effectiveness of REBOA zone 1 for AO in trauma resuscitation.
Conflict of interest statement
Figures
Comment in
-
Focused Empiricism and the Efficacy of Resuscitative Endovascular Balloon Occlusion of the Aorta.JAMA Surg. 2023 Feb 1;158(2):150-151. doi: 10.1001/jamasurg.2022.6430. JAMA Surg. 2023. PMID: 36542387 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
