

A modelling approach to hepatic glucose production estimation
- PMID: 36542610
- PMCID: PMC9770442
- DOI: 10.1371/journal.pone.0278837
A modelling approach to hepatic glucose production estimation
Abstract
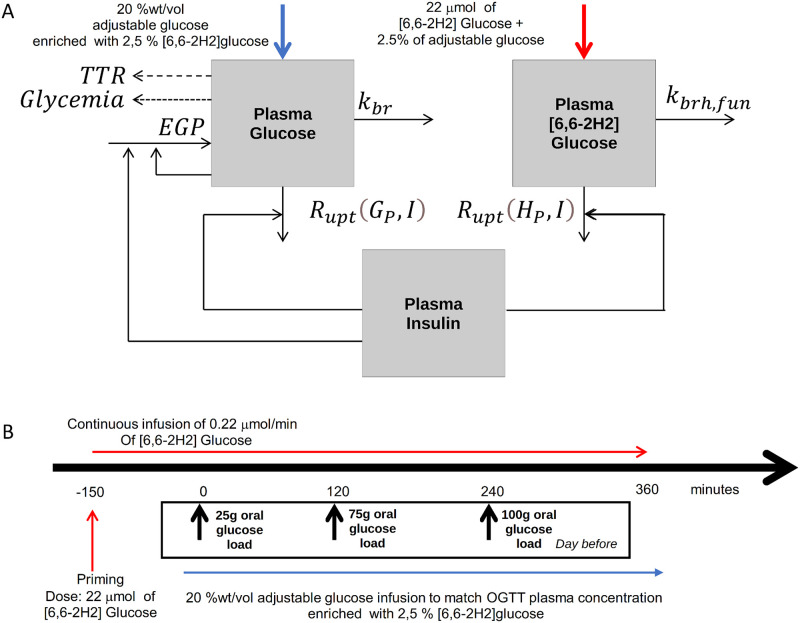
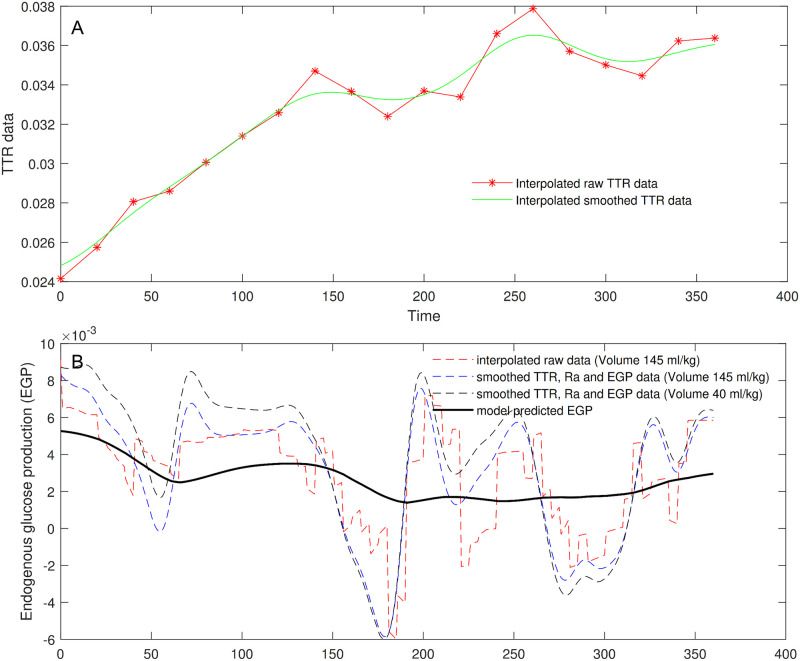
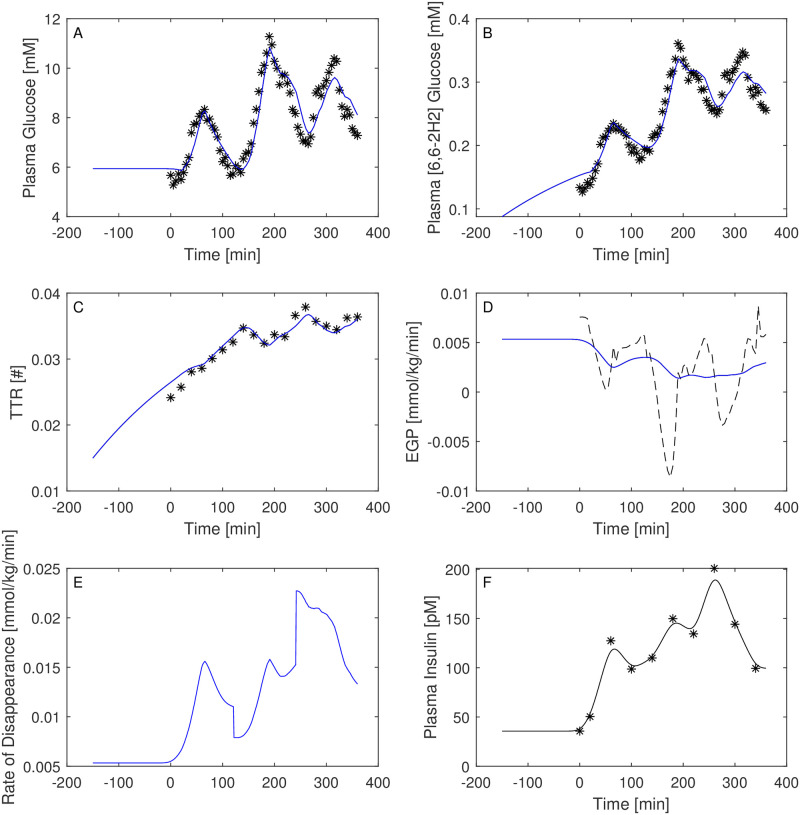
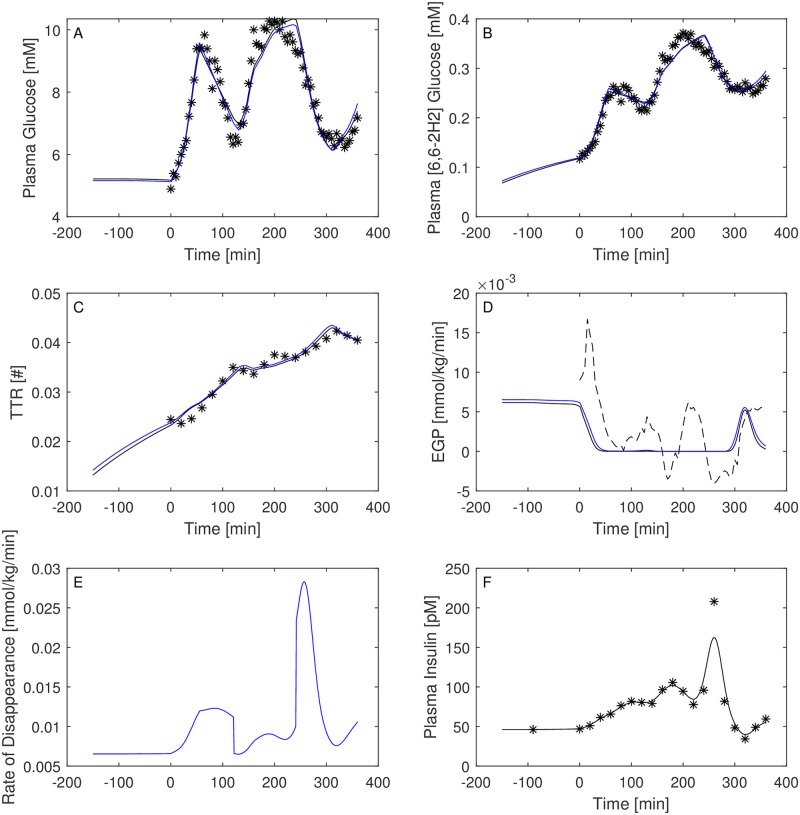
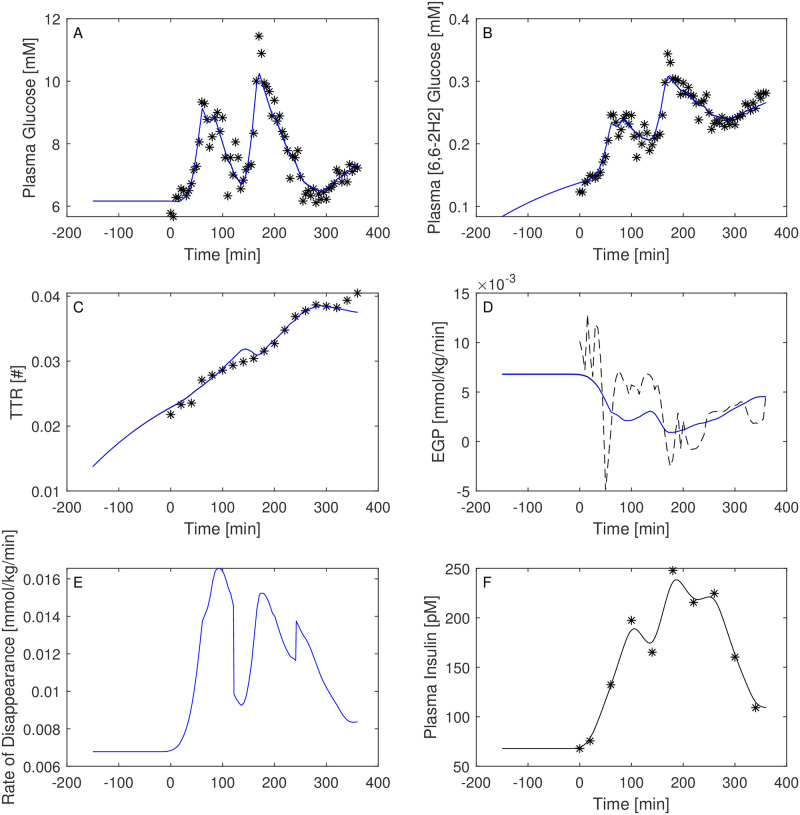
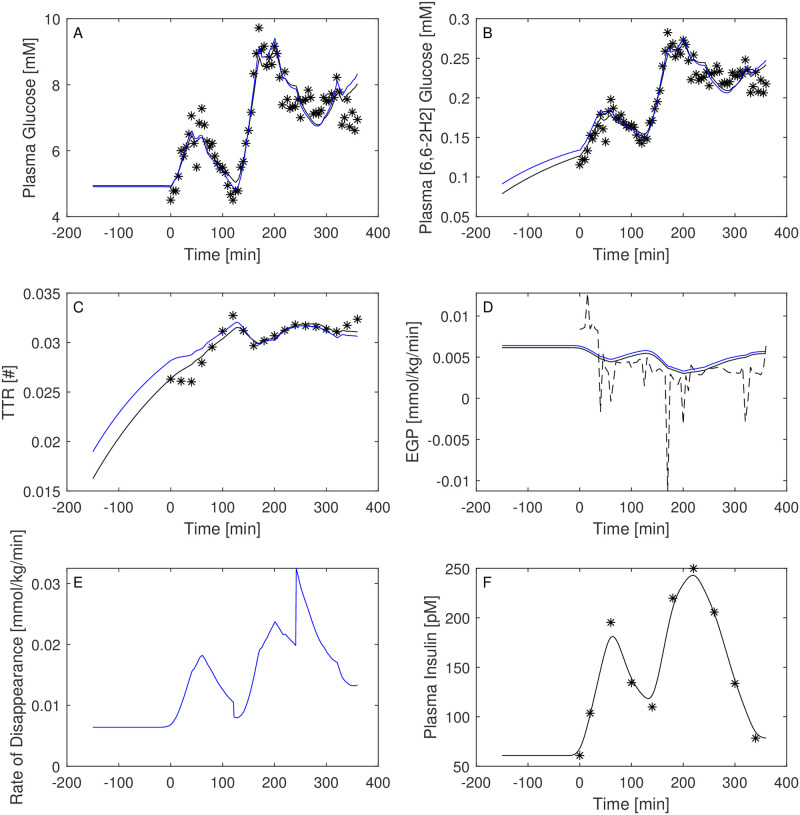
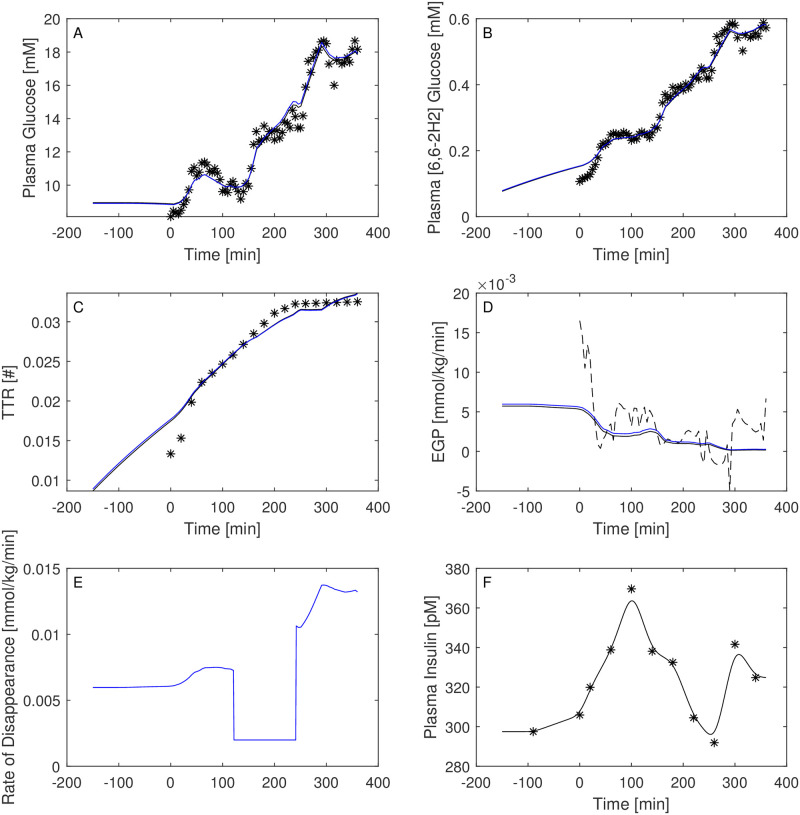
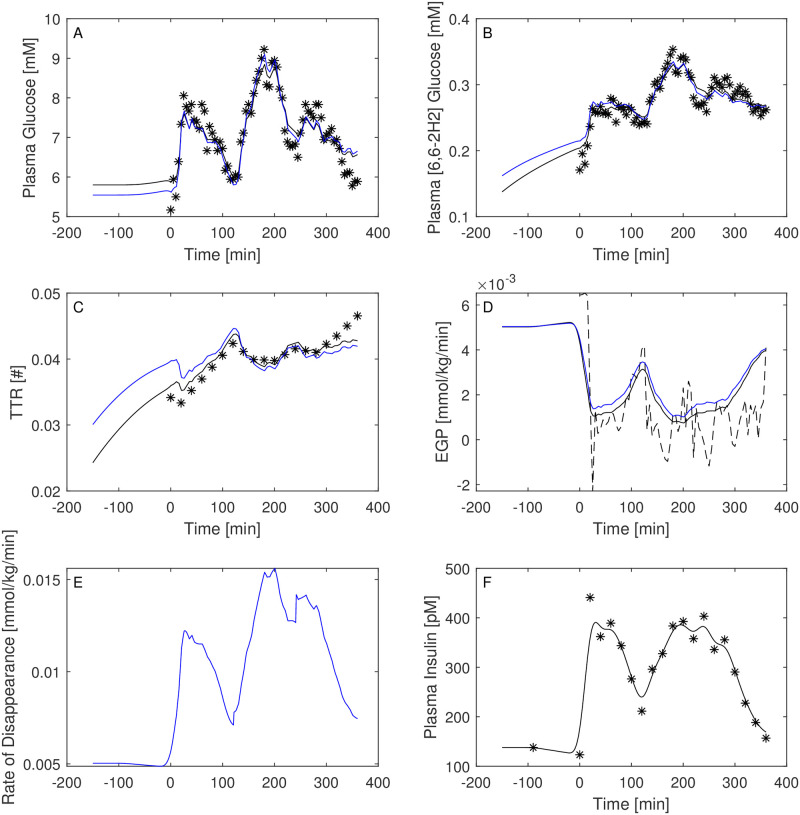
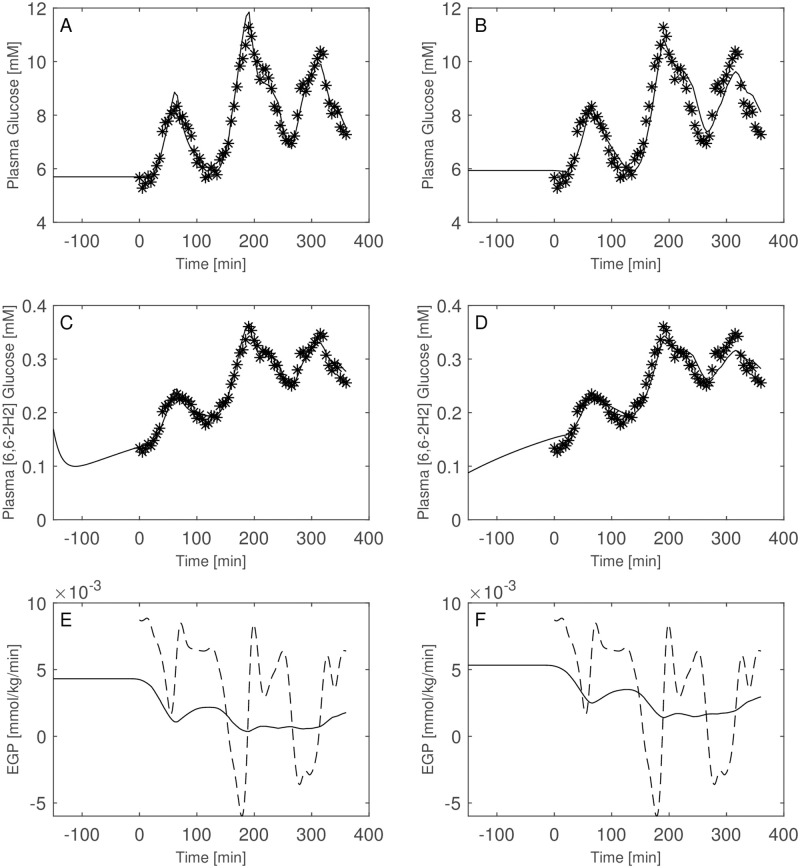
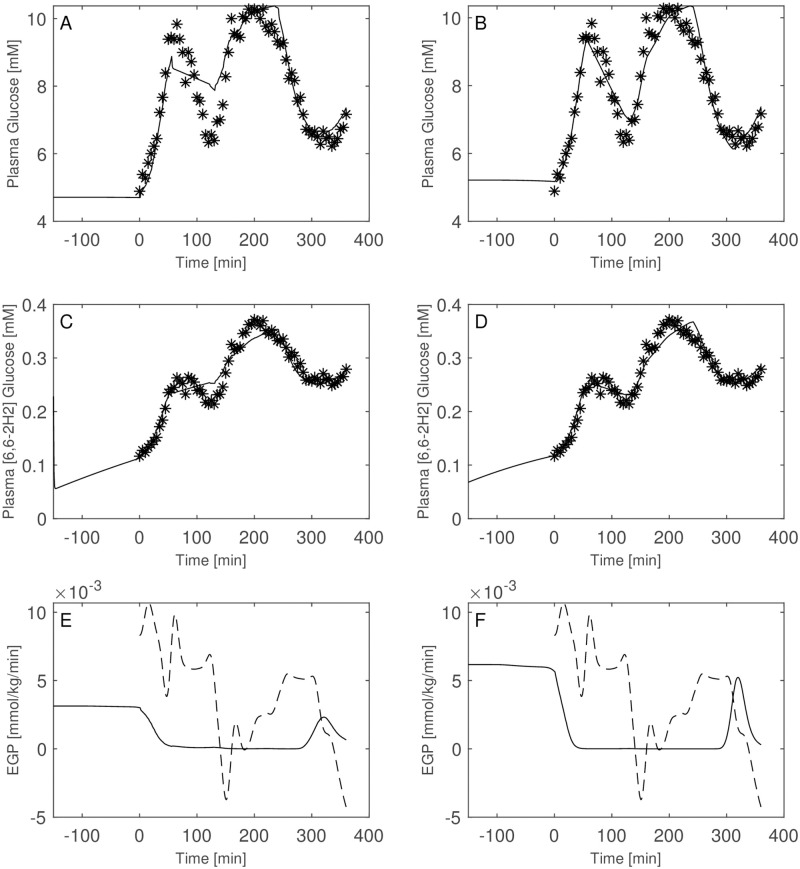
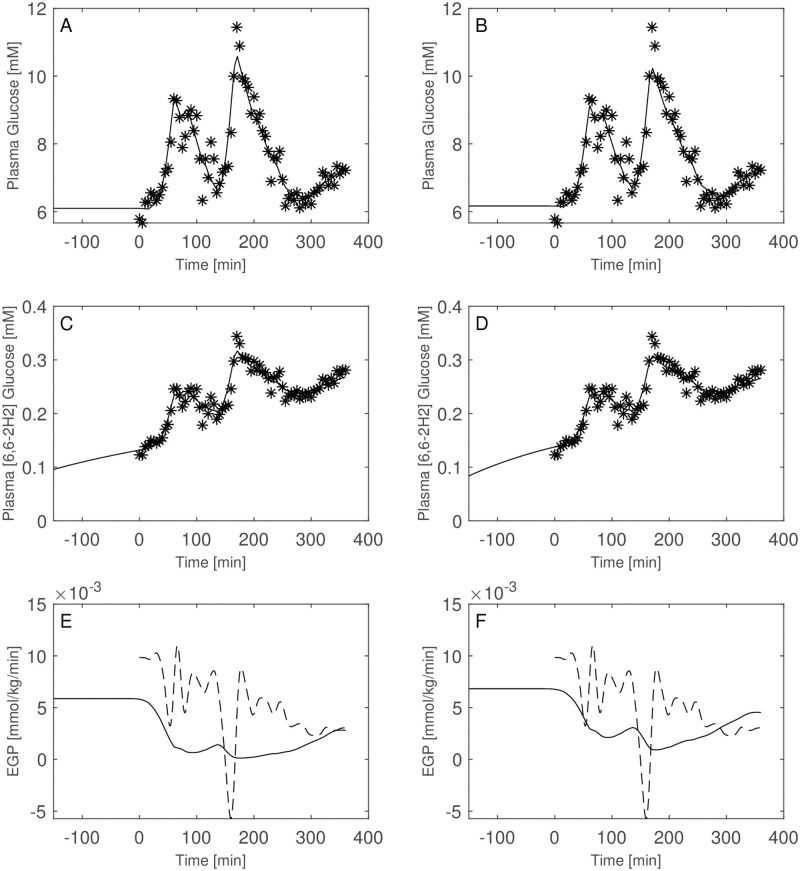
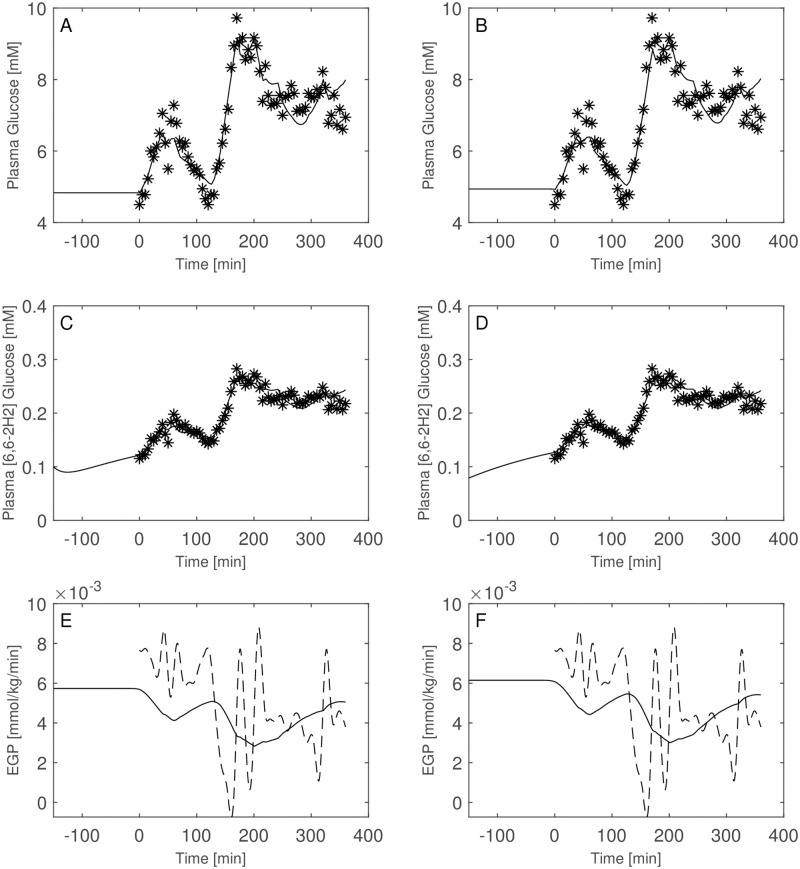
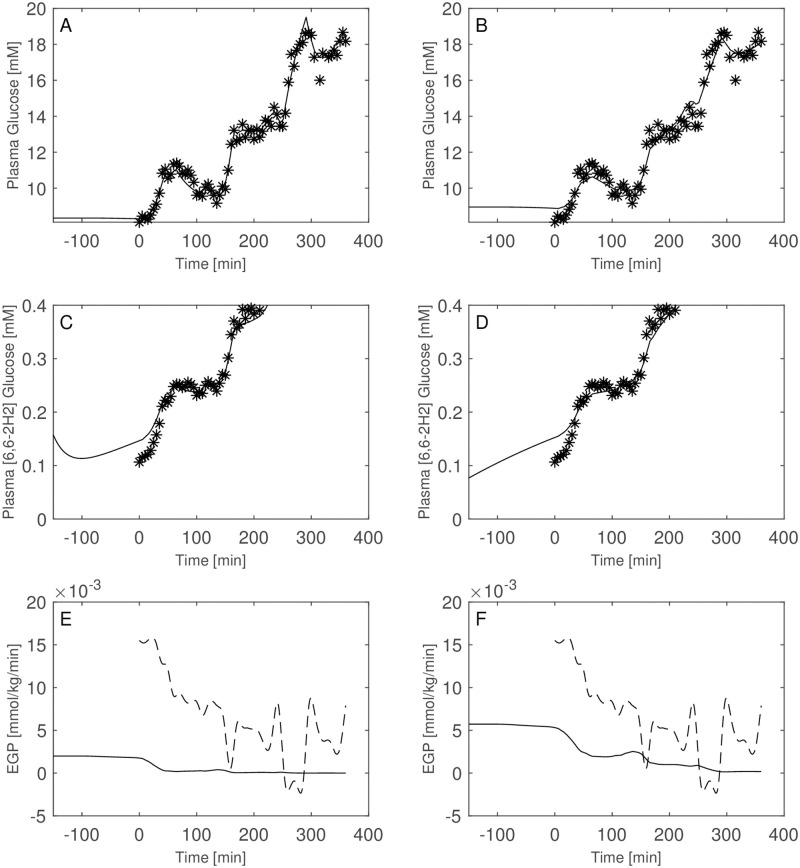
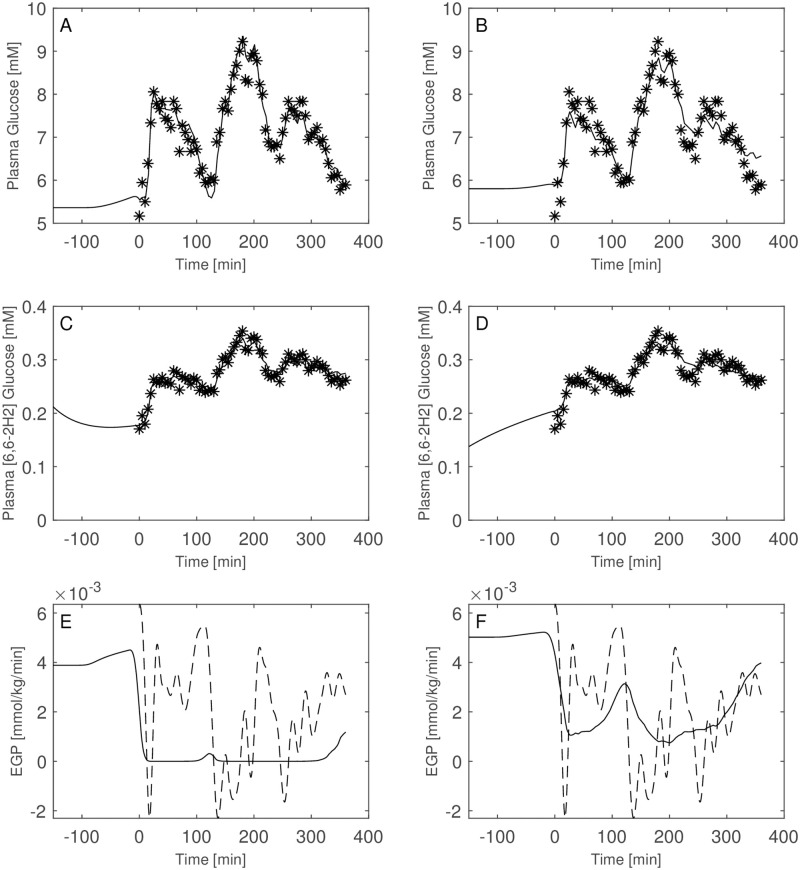
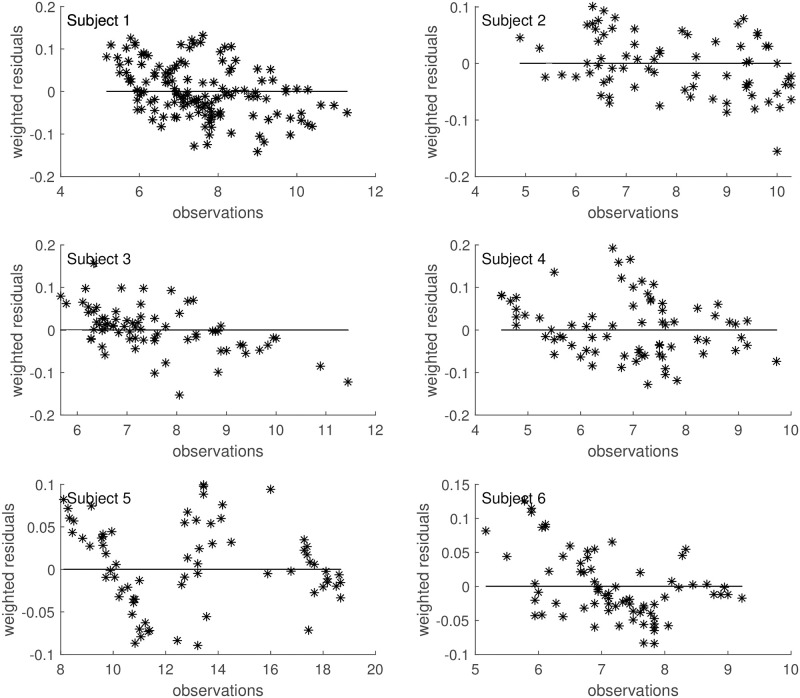
Stable isotopes are currently used to measure glucose fluxes responsible for observed glucose concentrations, providing information on hepatic and peripheral insulin sensitivity. The determination of glucose turnover, along with fasting and postprandial glucose concentrations, is relevant for inferring insulin sensitivity levels. At equilibrium (e.g. during the fasting state) the rate of glucose entering the circulation equals its rate of disappearance from the circulation. If under these conditions tracer is infused at a constant rate and Specific Activity (SA) or Tracer to Tracee (TTR) ratio is computed, the Rate of Appearance (RA) equals the Rate of Disappearance (RD) and equals the ratio between infusion rate and TTR or SA. In the post-prandial situation or during perturbation studies, however, estimation of RA and RD becomes more complex because they are not necessarily equal and, furthermore, may vary over time due to gastric emptying, glucose absorption, appearance of ingested or infused glucose, variations of EGP and glucose disappearance. Up to now, the most commonly used approach to compute RA, RD and EGP has been the single-pool model by Steele. Several authors, however, report pitfalls in the use of this method, such as "paradoxical" increase in EGP immediately after meal ingestion and "negative" rates of EGP. Different attempts have been made to reduce the impact of these errors, but the same problems are still encountered. In the present work a completely different approach is proposed, where cold and labeled [6, 6-2H2] glucose observations are simultaneously fitted and where both RD and EGP are represented by simple but reasonable functions. As an example, this approach is applied to an intra-venous experiment, where cold glucose is infused at variable rates to reproduce a desired glycaemic time-course. The goal of the present work is to show that appropriate, if simple, modelling of the whole infusion procedure together with the underlying physiological system allows robust estimation of EGP with single-tracer administration, without the artefacts produced by the Steele method.
Copyright: © 2022 Panunzi, De Gaetano. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Mingrone G, Panunzi S, De Gaetano A, Guidone C, Iaconelli A, et al.. (2004) Bariatric-metabolic surgery versus conventional medical treatment in obese patients with type 2 diabetes: 5 year follow-up of an open-label, single-centre, randomised controlled trial. Lancet 386: 964–973. doi: 10.1016/S0140-6736(15)00075-6 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
