

Genomic heterogeneity as a barrier to precision oncology in urothelial cancer
- PMID: 36543146
- PMCID: PMC9882421
- DOI: 10.1016/j.celrep.2022.111859
Genomic heterogeneity as a barrier to precision oncology in urothelial cancer
Abstract
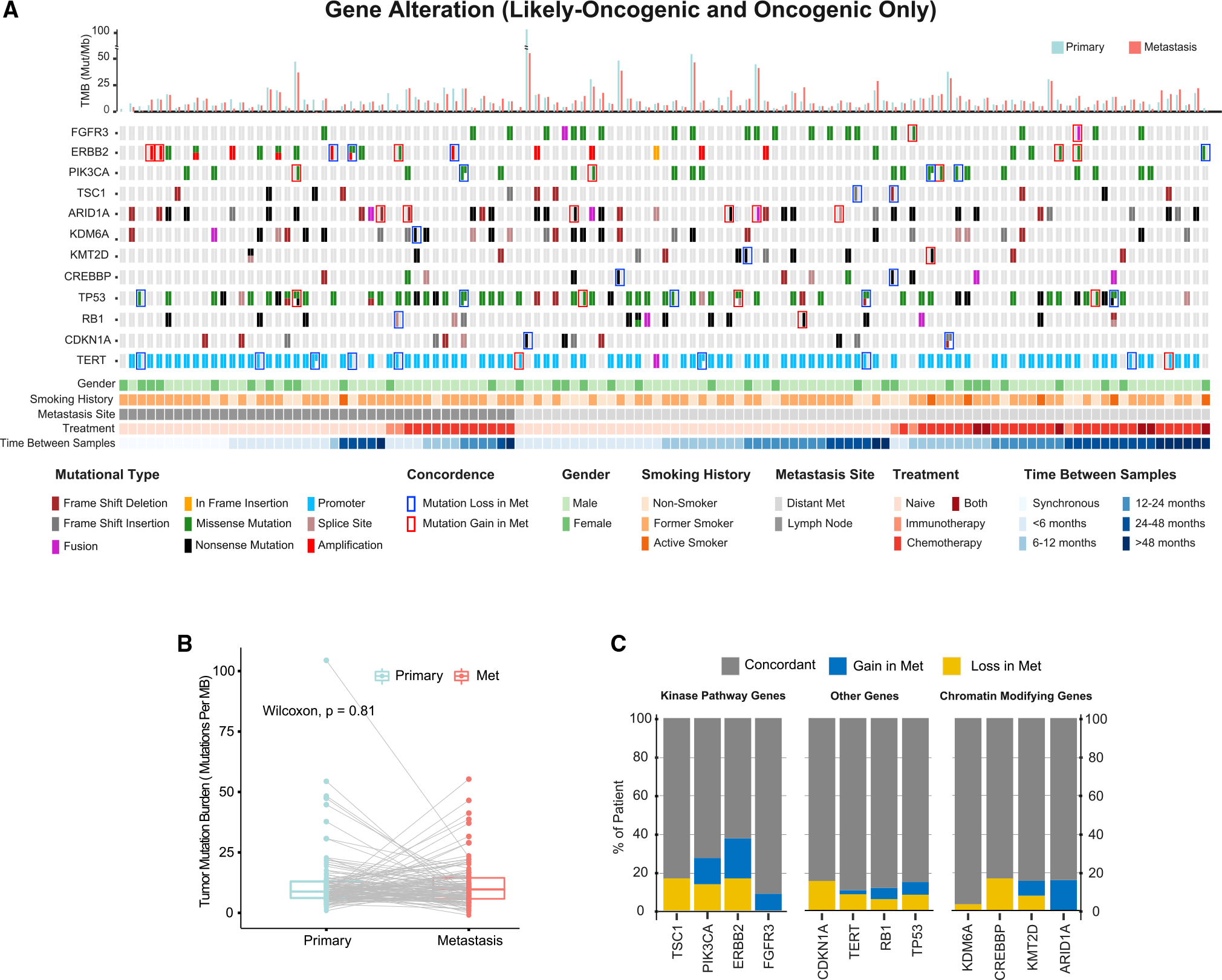
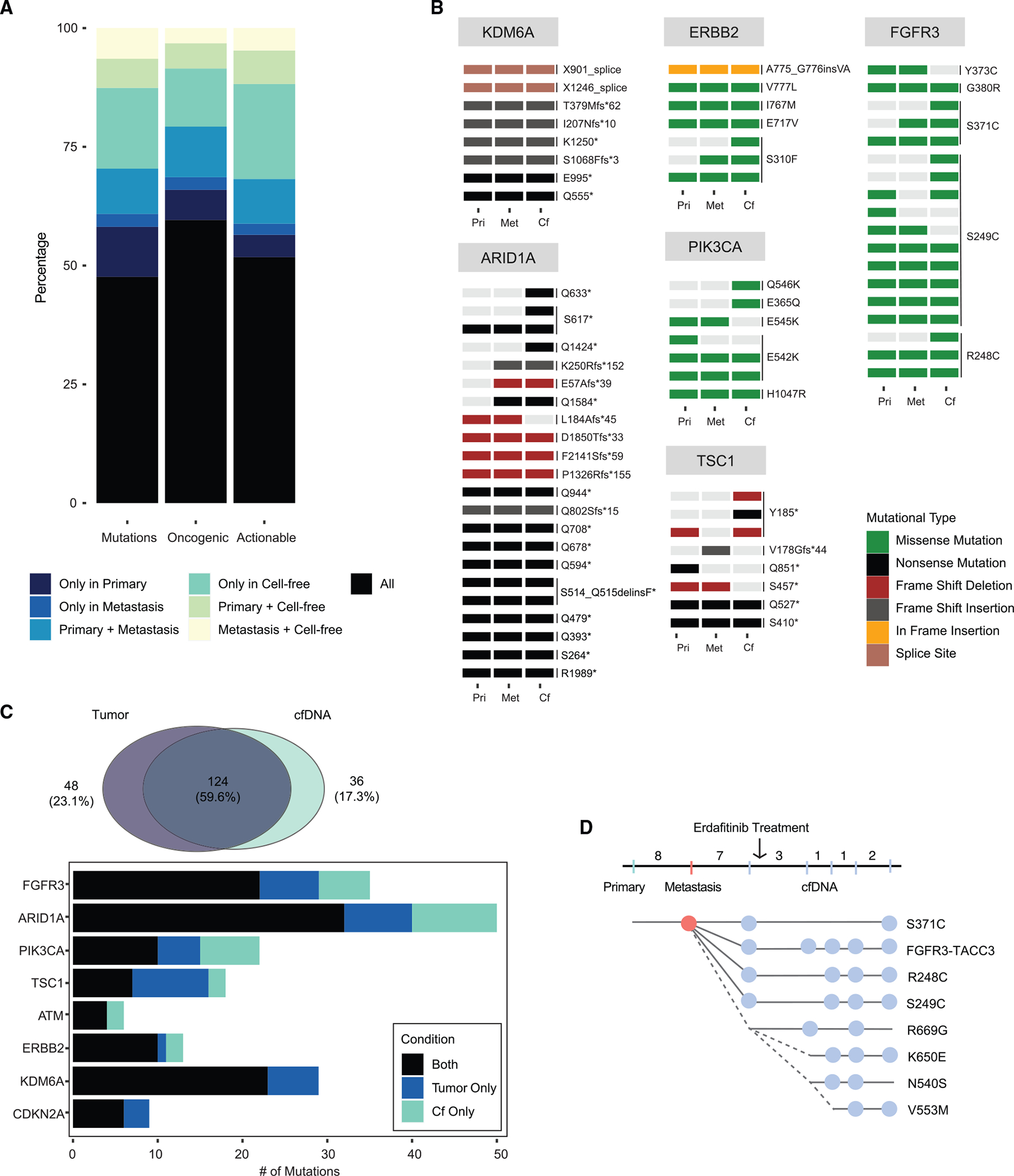
Precision oncology relies on the accurate molecular characterization of individual patients with cancer at the time of treatment initiation. However, tumor molecular profiles are not static, and cancers continually evolve because of ongoing mutagenesis and clonal selection. Here, we performed genomic analyses of primary tumors, metastases, and plasma collected from individual patients to define the concordance of actionable genomic alterations and to identify drivers of metastatic disease progression. We observed a high degree of discordance of actionable genomic alterations, with 23% discordant between primary and metastatic disease sites. Among chromatin-modifying genes, ARID1A mutations, when discordant, were exclusive to the metastatic tumor samples. Our findings indicate that the high degree of lesion-to-lesion genomic heterogeneity may be a barrier to precision oncology approaches for bladder cancer and that circulating tumor DNA profiling may be preferred to tumor sequencing for a subset of patients.
Keywords: ARID1A; CP: Cancer; FGFR3; bladder cancer; cell-free DNA; genomic heterogeneity; metastasis; urothelial carcinoma.
Copyright © 2022 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Author contributions Conceptualization, T.N.C., Z.C., H.W., S.C., H.A.A.-A., and D.B.S; methodology, T.N.C., Z.C., H.W., A.T.L., S.C., M.T.A.D., N.A., S.D., J.E.R., N.V., E.J.P., S.P.G., W.H., H.A.A.-A., and D.B.S.; investigation, T.N.C., Z.C., H.W., A.T.L., S.C., M.T.A.D., N.A., C.C., S.D., J.R., N.V., S.P.G., W.H., and H.A.A.-A.; resources, P.R., J.R., D.F.B., M.Y.T., B.H.B., M.B., E.J.P., G.I., H.A.A.-A., and D.B.S.; formal analysis, T.N.C., Z.C., A.T.L., S.C., M.T.A.D., I.O., and W.H.; writing, T.N.C., Z.C., A.T.L., and D.B.S.; review & editing, T.N.C., Z.C., H.A.A.-A., and D.B.S.; supervision, D.B.S. Declaration of interests D.B.S. has served as a consultant for/received honorarium from Pfizer, Loxo/Lilly Oncology, Vividion Therapeutics, Scorpion Therapeutics, Fore Therapeutics, FOG Pharma, Rain Therapeutics, and BridgeBio. H.A.A.-A. provided consultation to AstraZeneca, Janssen Biotech, Bristol-Myers-Squibb, and Paige.ai. J.E.R. has served as a consultant for Astellas, Seagen, Merck, Roche, Genentech, AstraZeneca, Janssen Biotech, Gilead, Pfizer, EMD-Serono, Mirati, Boehringer Ingelheim, Pharmacyclis, GSK, Infinity, Tyra BioSciences, Bayer, and QED Therapeutics and received honoraria from EMD-Serono. M.B. has served as a consultant for Eli Lilly and PetDx and has a patent pending on “Systems and Methods for Detecting Cancer Via cfDNA Screening.” S.D. has served as a consultant for Roche.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
