

Long-term multisystemic efficacy of migalastat on Fabry-associated clinical events, including renal, cardiac and cerebrovascular outcomes
- PMID: 36543533
- PMCID: PMC10359570
- DOI: 10.1136/jmg-2022-108669
Long-term multisystemic efficacy of migalastat on Fabry-associated clinical events, including renal, cardiac and cerebrovascular outcomes
Abstract
Background: Fabry disease is a rare, multisystemic disorder caused by GLA gene variants that lead to alpha galactosidase A deficiency, resulting in accumulation of glycosphingolipids and cellular dysfunction. Fabry-associated clinical events (FACEs) cause significant morbidity and mortality, yet the long-term effect of Fabry therapies on FACE incidence remains unclear.
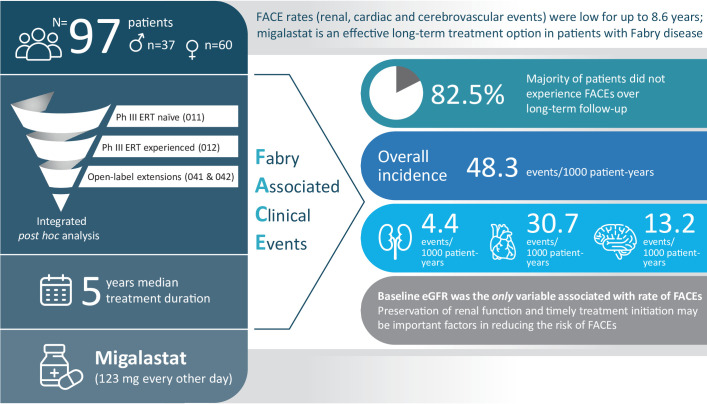
Methods: This posthoc analysis evaluated incidence of FACEs (as a composite outcome and separately for renal, cardiac and cerebrovascular events) in 97 enzyme replacement therapy (ERT)-naïve and ERT-experienced adults with Fabry disease and amenable GLA variants who were treated with migalastat for up to 8.6 years (median: 5 years) in Phase III clinical trials of migalastat. Associations between baseline characteristics and incidence of FACEs were also evaluated.
Results: During long-term migalastat treatment, 17 patients (17.5%) experienced 22 FACEs and there were no deaths. The incidence rate of FACEs was 48.3 events per 1000 patient-years overall. Numerically higher incidence rates were observed in men versus women, patients aged >40 years versus younger patients, ERT-naïve versus ERT-experienced patients and men with the classic phenotype versus men and women with all other phenotypes. There was no statistically significant difference in time to first FACE when analysed by patient sex, phenotype, prior treatment status or age. Lower baseline estimated glomerular filtration rate (eGFR) was associated with an increased risk of FACEs across patient populations.
Conclusions: The overall incidence of FACEs for patients during long-term treatment with migalastat compared favourably with historic reports involving ERT. Lower baseline eGFR was a significant predictor of FACEs.
Keywords: Cardiovascular Diseases; Cerebrovascular Disorders; Genetics, Medical; Mutation.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: DAH reports advisory board participation, consulting fees and honoraria for Takeda, Sanofi, Amicus Therapeutics, Inc., Idorsia, Freeline and Protalix. DGB reports advisory board participation, consulting fees, speakers’ bureau fees and honoraria from Amicus Therapeutics, Inc. and Sanofi/Genzyme. RG reports consulting fees from Abeona, Amicus Therapeutics, Inc., Chiesi, Denali, Inventiva, JCR, Novartis, PTC, Protalix, RegenxBio and Sobi; speakers’ bureau fees from BioMarin, Amicus Therapeutics, Inc., Chiesi, Idorsia, Janssen, Novartis, Pfizer, PTC, Sanofi and Takeda; research funding from Allievex, Avrobio, Azafaros, JCR, Lysogene, Paradigm, PassageBio, RegenxBio, Sanofi, Sigilon, Takeda and Ultragenyx. RJH reports consulting fees from Alexion, Amicus Therapeutics, Inc., Avrobio, Chiesi, Sangamo, Sanofi/Genzyme and Takeda; advisory fees from Alexion, Amicus Therapeutics, Inc. and Sanofi/Genzyme; speakers’ bureau fees from Alexion and Sanofi/Genzyme and grants/research funding from Alexion, Amicus Therapeutics, Inc., Idorsia, Protalix, Sangamo, Sanofi/Genzyme and Takeda. EK reports consulting fees from Amicus Therapeutics, Inc. KN reports advisory board participation for Amicus Therapeutics, Inc., Takeda and Sanofi/Genzyme; consulting fees from Amicus Therapeutics, Inc. and Takeda and research funding from Amicus Therapeutics, Inc., Takeda, Sanofi/Genzyme, Idorsia and Avrobio. IO reports advisory board participation for Amicus Therapeutics, Inc., Bristol Myers Squibb, Bayer, Astra Zeneca and Cytokinetics; contracted research for Amicus Therapeutics, Inc., Menarini International, Shire-Takeda, Bristol Myers Squibb, Boston Scientific and Sanofi/Genzyme and speaker’s bureau fees from Boston Scientific, Bristol Myers Squibb and Sanofi/Genzyme. UF-R reports advisory board participation from Amicus Therapeutics, Inc., Freeline, Sanofi/Genzyme and Takeda; speakers’ fees and travel support from Amicus Therapeutics, Inc., Sanofi/Genzyme and Takeda and research funding from Sanofi/Genzyme and Takeda. NSa reports speakers’ bureau fees from Amicus Therapeutics, Inc., Takeda, JCR and Sanofi and research funding from JCR and Sanofi. NSk was an employee and stockholder in Amicus Therapeutics, Inc. at the time of drafting this manuscript and determining the analysis plan. GS-P reports advisory board participation for Amicus Therapeutics, Inc. and Sanofi, research grants/funding from Amicus Therapeutics, Takeda, Idorsia and Freeline and honoraria from Amicus Therapeutics, Inc. and Sanofi. RT reports advisory board participation, consulting fees and honoraria for Takeda, Sanofi, Amicus Therapeutics, Inc. and Chiesi. WRW reports advisory board participation for Sanofi/Genzyme, Takeda, Chiesi, Alexion/Astra Zeneca and BioMarin; research funding from Amicus Therapeutics, Inc. and Takeda; consulting fees from Amicus Therapeutics, Inc. and Spark; contracted clinical study research from Amicus Therapeutics, Inc., Alexion/Astra Zeneca, BioMarin, Chiesi, Freeline, Orphazyme, Pfizer, Protalix, Sangamo, Sanofi/Genzyme, Takeda and 4D Molecular Therapeutics.
Figures



References
-
- Ortiz A, Germain DP, Desnick RJ, Politei J, Mauer M, Burlina A, Eng C, Hopkin RJ, Laney D, Linhart A, Waldek S, Wallace E, Weidemann F, Wilcox WR. Fabry disease revisited: management and treatment recommendations for adult patients. Mol Genet Metab 2018;123:416–27. 10.1016/j.ymgme.2018.02.014 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous