

Real-world usage of digital health applications (DiGA) in rheumatology: results from a German patient survey
- PMID: 36543961
- PMCID: PMC9770561
- DOI: 10.1007/s00296-022-05261-7
Real-world usage of digital health applications (DiGA) in rheumatology: results from a German patient survey
Abstract
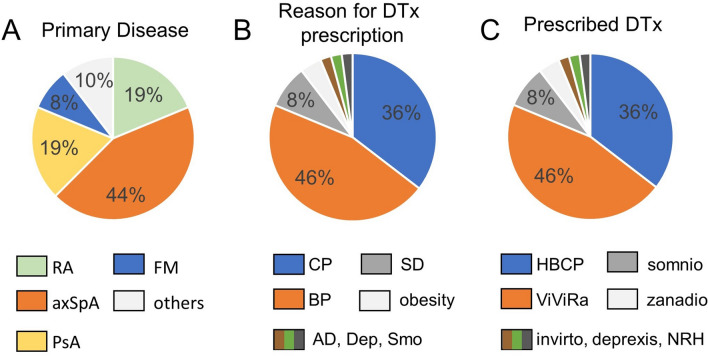
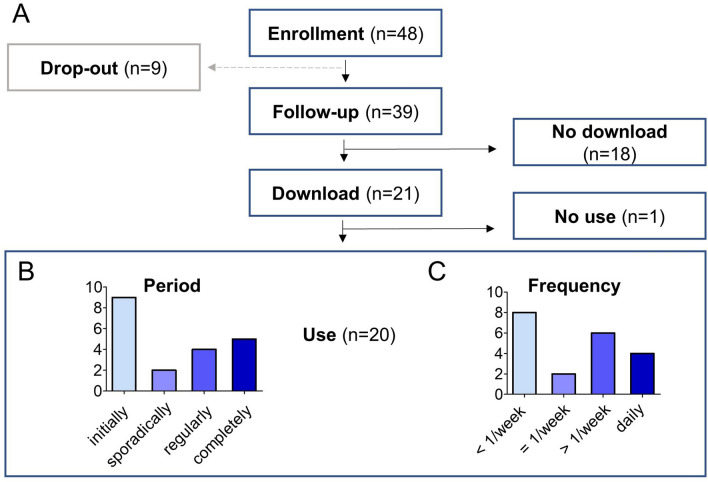
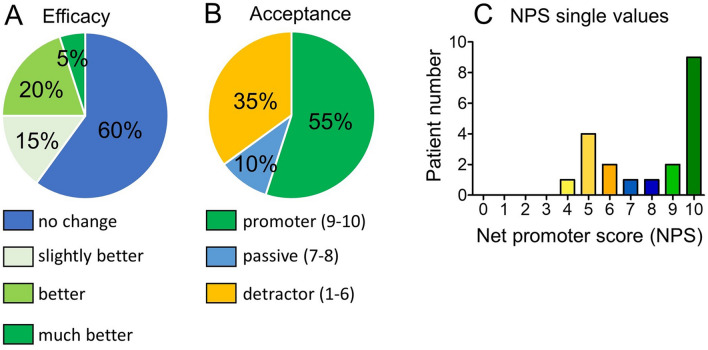
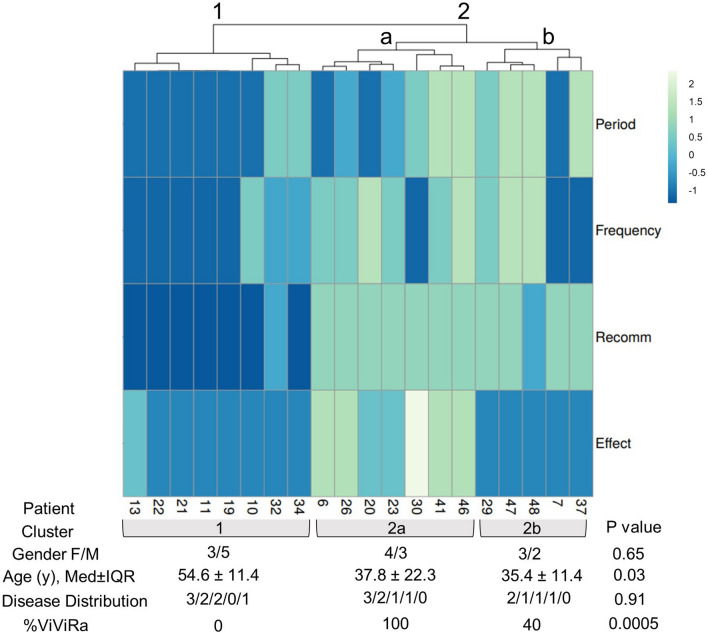
Mobile health applications and digital therapeutics (DTx) aim to improve current patient care. Real-world data on DTx are, however, scarce. The aim of this study was to evaluate the adherence, acceptance, and efficacy of DTx in a clinical routine rheumatology setting. We conducted a prospective observational cohort study assessing the use, adherence, acceptance, and efficacy of the DTx DiGA (Digitale Gesundheitsanwendungen) by survey over 12 weeks. Patients included had to have a rheumatic disease and had been prescribed a DiGA. Acceptance was assessed using the Net promoter score (NPS). 48 patients were prescribed DiGA. Of these, 39/48 (81%) completed the follow-up survey. 21/39 (54%) patients downloaded the DTx and 20/39 (51%) used the DTx at least once. 9/39 (23%) of patients stopped quickly afterward and 5/39 (13%) reported having completed the whole DTx program. Lack of time and commitment were reported as the main reasons for non-use. Overall acceptance of DiGA was high (Net promoter score (NPS) mean (SD) 7.8/10 (2.3)). While the majority of patients (60%) reported no improvement, one subgroup of patients (7/20, 35%) who regularly used an exercise-based DTx for back pain reported symptom improvement. Acceptance of DTx in patients with rheumatic diseases is high, however onboarding to DTx use and adherence to DTx is still challenging in patients with rheumatic diseases. In a subgroup of patients with back pain, however, the use of an exercise-based DTx led to symptom improvement.
Keywords: Adherence; Apps; DTx; Digital health; Digital therapeutics; Interviews; Questionnaire; Survey; eHealth.
© 2022. The Author(s).
Conflict of interest statement
JK reports consultancy fees from ABATON GmbH and VILA Health. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
