

The point-of-care D-dimer test provides a fast and accurate differential diagnosis of Stanford Type A aortic syndrome and ST-elevated myocardial infarction in emergencies
- PMID: 36544083
- PMCID: PMC9768940
- DOI: 10.1186/s12872-022-02925-x
The point-of-care D-dimer test provides a fast and accurate differential diagnosis of Stanford Type A aortic syndrome and ST-elevated myocardial infarction in emergencies
Abstract
Background: The research of the sensitivity and specificity point-of-care testing (POCT) of D-dimer as a diagnostic protocol for differential diagnosis of Stanford Type A aortic syndrome (hereafter as TAAS) mimicking ST-elevated myocardial infarction (STEMI) with regular STEMI in the emergency department is limited.
Methods: Full medical information of 32 patients confirmed TAAS and 527 patients confirmed STEMI from January 1st, 2016 to October 1st, 2021 were retrospectively analyzed in Shanghai Tenth People's Hospital of Tongji University.
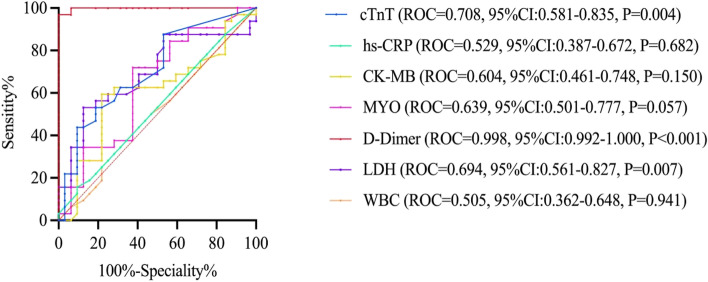
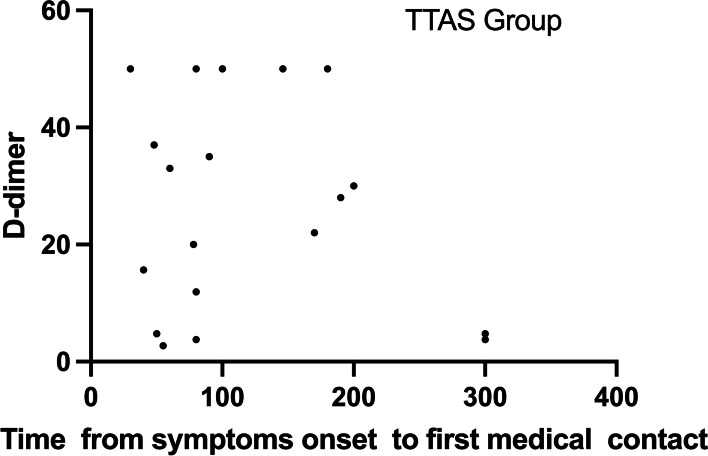
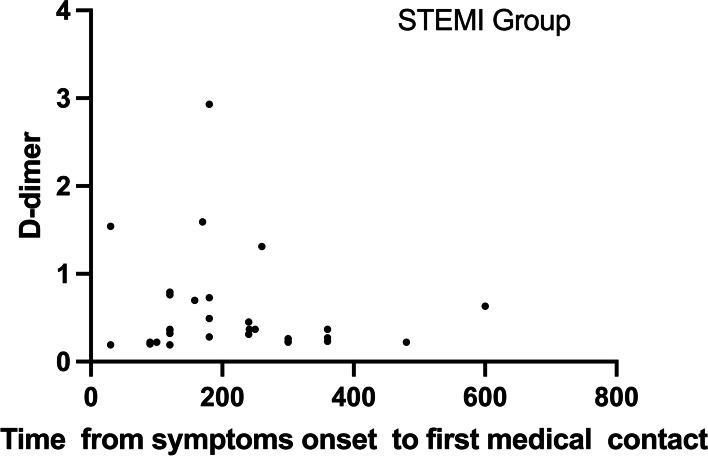
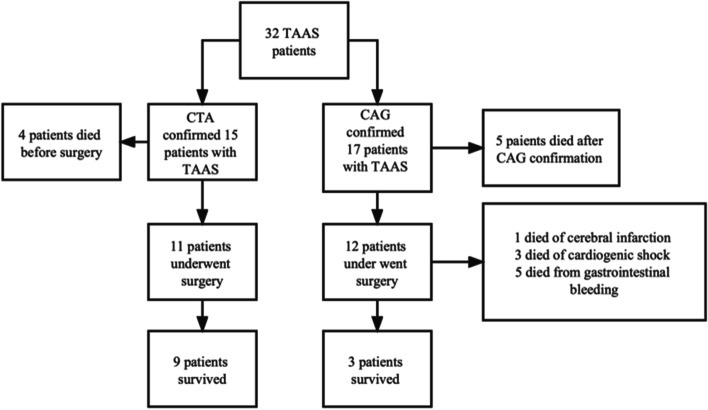
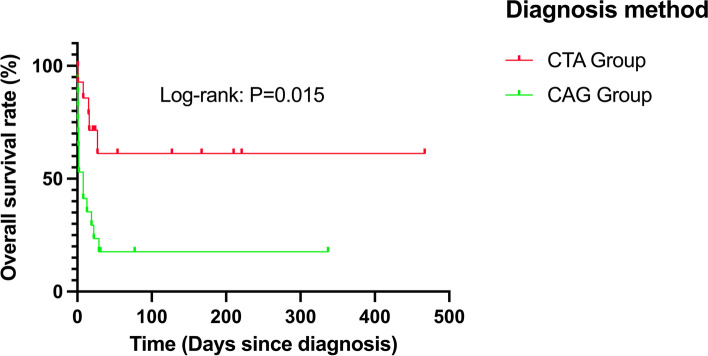
Results: The baseline characteristics of two groups of patients were well-balanced post propensity score matching (PSM) analysis, and each group had 32 patients enrolled. Patients in the STEMI group had higher positive cardiac troponin I (cTNI) (0.174 ng/ml vs. 0.055 ng/ml, P = 0.008) results but lower D-dimer (0.365μg/ml vs. 31.50μg/ml, P < 0.001) results than the TAAS group. The D-dimer cutoff value of 2.155μg/ml had the best sensitivity of 100% and specificity of 96.9%, and the positive predictive value (PPV) as well as the negative predictive value (NPV) of the cutoff value were 96.9 and 100%, respectively, in total 64 patients, the area under the curve (AUC) values were 0.998 (95% CI:0.992-1.000, P < 0.001) for the D-dimer. No significant correlation between the D-dimer concentration and the time from symptoms onset to first medical contact in both groups (TAAS group: r = - 0.248, P = 0.170; STEMI group: r = - 0.159, P = 0.383) or significant correlation between D-dimer and creatine clearance (TAAS group: r = - 0.065, P = 0.765; STEMI group: r = 0.222, P = 0.221). The total in-hospital mortality for the patients with TAAS presenting as STEMI was 62.5% (20/32). The mortality rate for TAAS patients confirmed by computed tomography angiography (CTA) was significantly lower (40% vs. 82.4%, P = 0.014) than the mortality rate for TAAS patients confirmed by coronary angiography (CAG) and had a longer average survival time (log-rank = 0.015), less peri-surgical complications especially gastrointestinal hemorrhage (0.00% vs. 55.6%, P < 0.001). CTA diagnosis can reduce the mortality rate by 67.5% (95%CI:0.124-0.850, P = 0.16).
Conclusions: The POCT D-dimer with cut-off 2.155μg/ml would be useful to rule-out TAAS mimicking STEMI from regular STEMI prior to reperfusion therapy. CTA diagnosis is effective in reducing the probability of perioperative complications and lowering perioperative mortality than CAG diagnosis in TAAS patients.
Keywords: Coronary reperfusion therapy; D-dimer; ST-segment elevated myocardial infarction; Stanford type A aortic syndrome.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
D-dimer for screening of aortic dissection in patients with ST-elevation myocardial infarction.Am J Emerg Med. 2022 Sep;59:146-151. doi: 10.1016/j.ajem.2022.07.024. Epub 2022 Jul 16. Am J Emerg Med. 2022. PMID: 35868207
-
[The value of D-dimer for etiological diagnosis of mortal chest pain: an analysis of 438 cases].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2013 Nov;25(11):655-9. doi: 10.3760/cma.j.issn.2095-4352.2013.11.005. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2013. PMID: 24225209 Chinese.
-
Diagnostic performance and predictive value of D-dimer testing in patients referred to the emergency department for suspected myocardial infarction.Clin Biochem. 2022 Jun;104:22-29. doi: 10.1016/j.clinbiochem.2022.02.003. Epub 2022 Feb 15. Clin Biochem. 2022. PMID: 35181290
-
[Comparison of the predictive value of the modified CADILLAC, GRACE and TIMI risk scores for the risk of short-term death in patients with acute ST segment elevation myocardial infarction after percutaneous coronary intervention].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Mar;35(3):299-304. doi: 10.3760/cma.j.cn121430-20220727-00696. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 36916344 Chinese.
-
Prehospital diagnosis of patients with acute myocardial infarction.Diagnosis (Berl). 2016 Dec 1;3(4):155-166. doi: 10.1515/dx-2016-0021. Diagnosis (Berl). 2016. PMID: 29536903 Review.
Cited by
-
A Novel Tool for Distinguishing Type A Acute Aortic Syndrome from Heart Failure and Acute Coronary Syndrome.Diagnostics (Basel). 2023 Nov 18;13(22):3472. doi: 10.3390/diagnostics13223472. Diagnostics (Basel). 2023. PMID: 37998608 Free PMC article.
References
-
- Fan QK, Wang WW, Zhang ZL, Liu ZJ, Yang J, Zhao GS, et al. Evaluation of D-dimer in the diagnosis of suspected aortic dissection. Clin Chemistry Laboratory Med. 2010;48:1733–7. - PubMed
-
- Anderson JL. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: A report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;127. - PubMed
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) European Heart J. 2018;39:119–177. doi: 10.1093/eurheartj/ehx393. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
