

Postoperative complications and oncologic outcomes after multimodal therapy of localized high risk soft tissue sarcoma
- PMID: 36544149
- PMCID: PMC9768905
- DOI: 10.1186/s13014-022-02166-4
Postoperative complications and oncologic outcomes after multimodal therapy of localized high risk soft tissue sarcoma
Abstract
Background: Standard therapy for localized high-risk soft tissue sarcoma includes surgical resection and neoadjuvant or adjuvant radiation therapy (± chemotherapy and locoregional hyperthermia). No difference in oncologic outcomes for patients treated with neoadjuvant and adjuvant radiation therapy was reported, whereas side effect profiles differ. The aim of this analysis was to analyse oncologic outcomes and postoperative complications in patients treated with multimodal treatment.
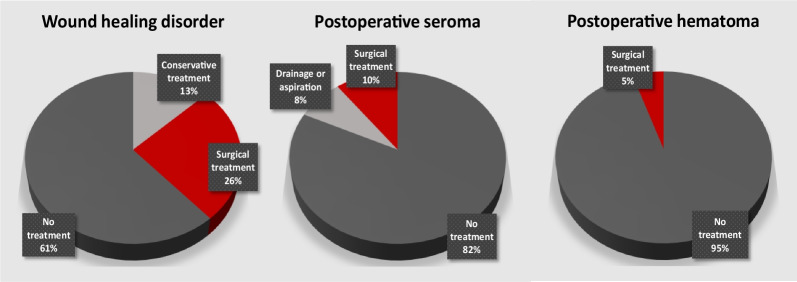
Methods: Oncologic outcomes and major wound complications (MWC, subclassified as wound healing disorder, infection, abscess, fistula, seroma and hematoma) were evaluated in 74 patients with localized high-risk soft tissue sarcoma of extremities and trunk undergoing multimodal treatment, and also separately for the subgroup of lower extremity tumors. Clinical factors and treatment modalities (especially neoadjuvant vs. adjuvant radiotherapy) were evaluated regarding their prognostic value and impact on postoperative wound complications.
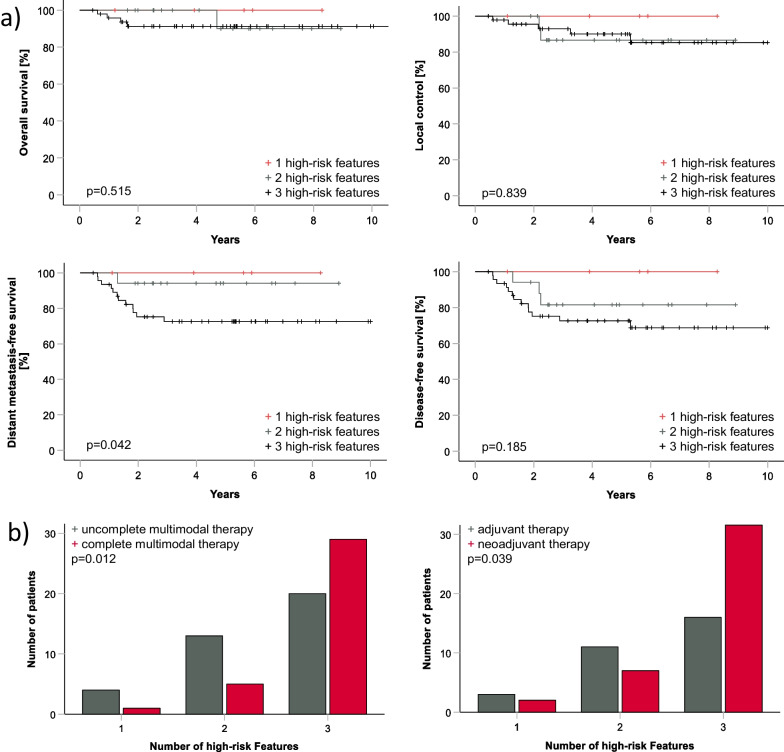
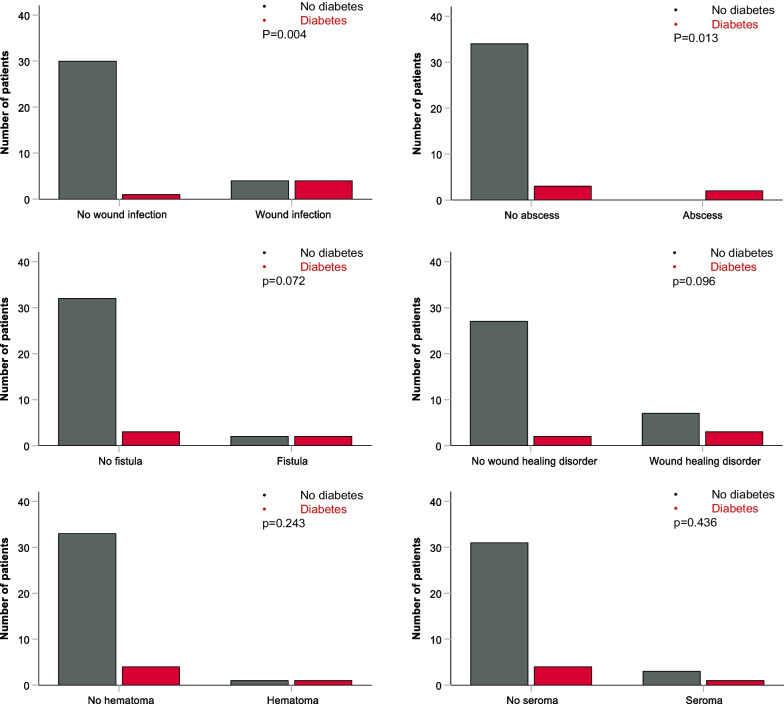
Results: Oncologic outcomes were dependent on number of high risk features (tumor size, depth to superficial fascia and grading), but not on therapy sequencing (however with higher risk patients in the neoadjuvant group). Different risk factors influenced different subclasses of wound healing complications. Slightly higher MWC-rates were observed in patients treated with neoadjuvant therapy, compared to adjuvant radiotherapy, although only with a trend to statistical significance (31.8% vs. 13.3%, p = 0.059). However, except for wound infections, no significant difference for other subclasses of postoperative complications was observed between neoadjuvant and adjuvant therapy. Diabetes was confirmed as a major risk factor for immune-related wound complications.
Conclusion: Rates of major wound complications in this cohort are comparable to published data, higher rates of wound infections were observed after neoadjuvant radiotherapy. Tumor localization, patient age and diabetes seem to be major risk factors. The number of risk factors for high risk soft tissue sarcoma seem to influence DMFS. Neoadjuvant treatment increases the risk only for wound infection treated with oral or intravenous antibiotic therapy and appears to be a safe option at an experienced tertiary center in absence of other risk factors.
Keywords: Multimodal therapy; Postoperative complications; Radiotherapy; Soft tissue sarcoma.
© 2022. The Author(s).
Conflict of interest statement
VP, CG, DZ, FP and FE have research and educational grants from Elekta, Philips, Siemens, Sennewald. The other authors declare that they have no conflict of interest.
Figures

References
-
- ESMO/European Sarcoma Network Working Soft tissue and visceral sarcomas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2014;25(Suppl 3):iii102–12. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
