

Comparative Effectiveness and Safety of Seizure Prophylaxis Among Adults After Acute Ischemic Stroke
- PMID: 36544249
- PMCID: PMC9870933
- DOI: 10.1161/STROKEAHA.122.039946
Comparative Effectiveness and Safety of Seizure Prophylaxis Among Adults After Acute Ischemic Stroke
Abstract
Background: Older adults occasionally receive seizure prophylaxis in an acute ischemic stroke (AIS) setting, despite safety concerns. There are no trial data available about the net impact of early seizure prophylaxis on post-AIS survival.
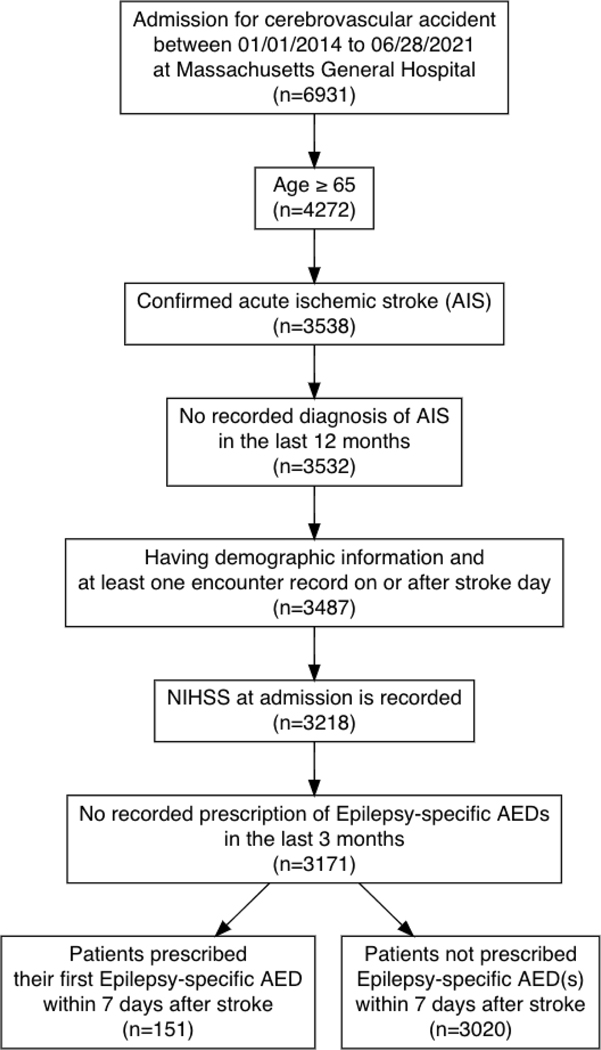
Methods: Using a stroke registry (American Heart Association's Get With The Guidelines) individually linked to electronic health records, we examined the effect of initiating seizure prophylaxis (ie, epilepsy-specific antiseizure drugs) within 7 days of an AIS admission versus not initiating in patients ≥65 years admitted for a new, nonsevere AIS (National Institutes of Health Stroke Severity score ≤20) between 2014 and 2021 with no recorded use of epilepsy-specific antiseizure drugs in the previous 3 months. We addressed confounding by using inverse-probability weights. We performed standardization accounting for pertinent clinical and health care factors (eg, National Institutes of Health Stroke Severity scale, prescription counts, seizure-like events).
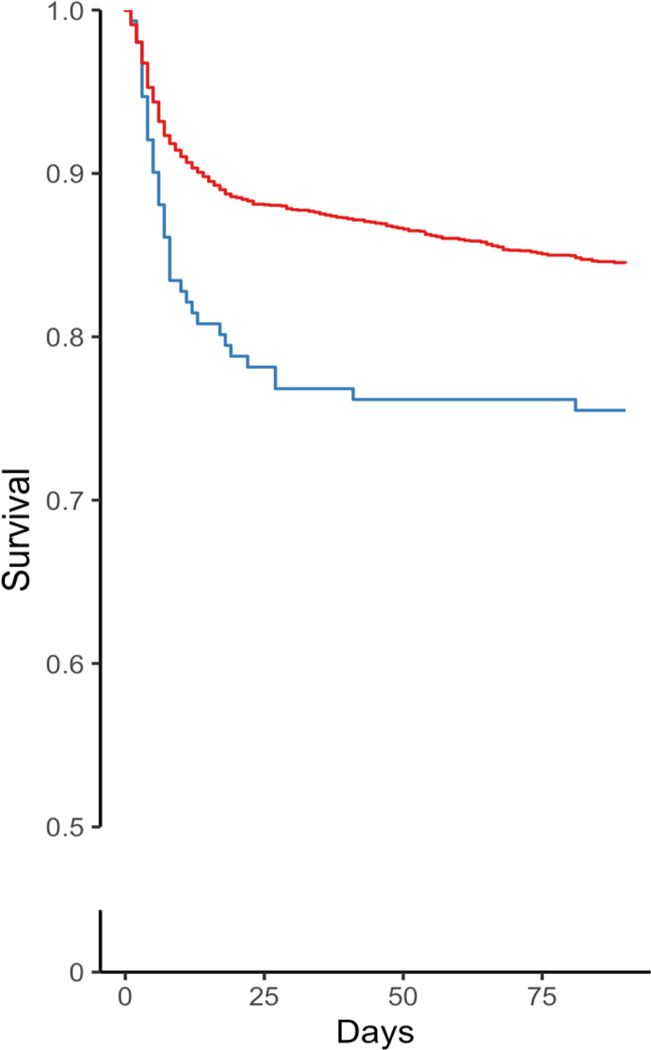
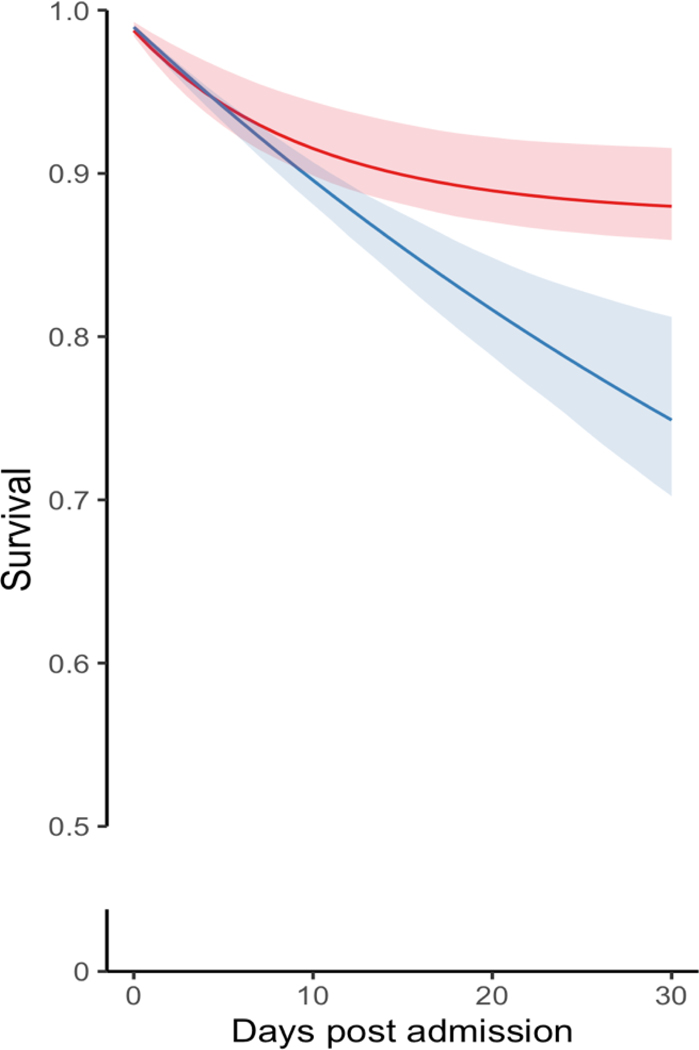
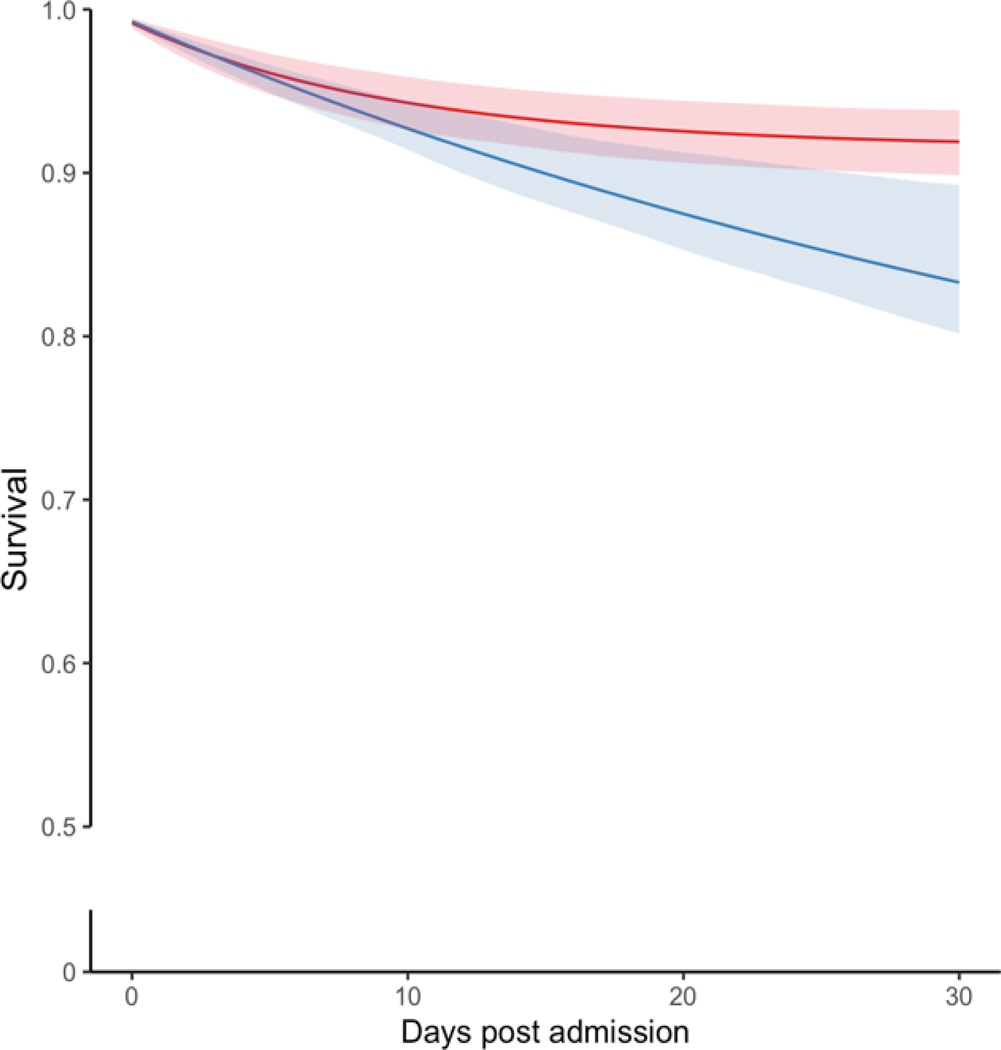
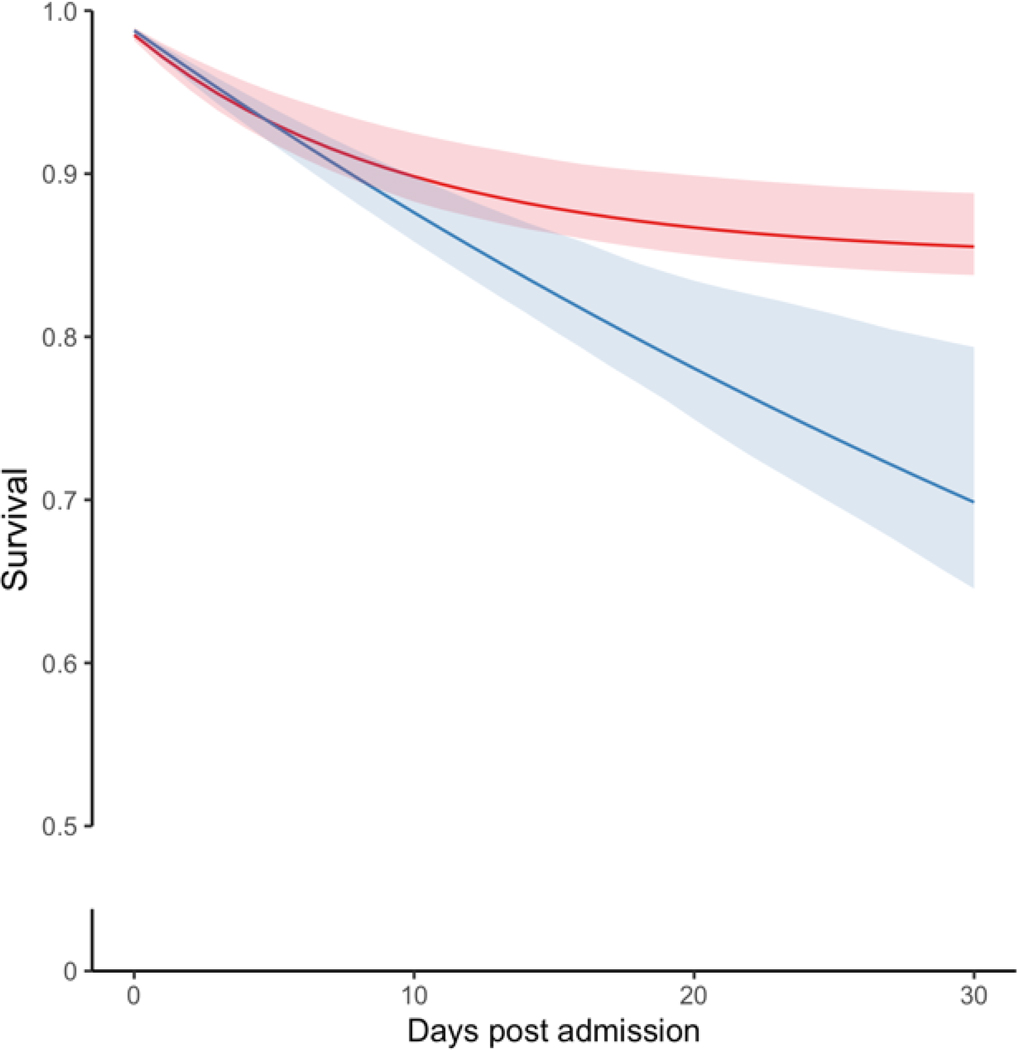
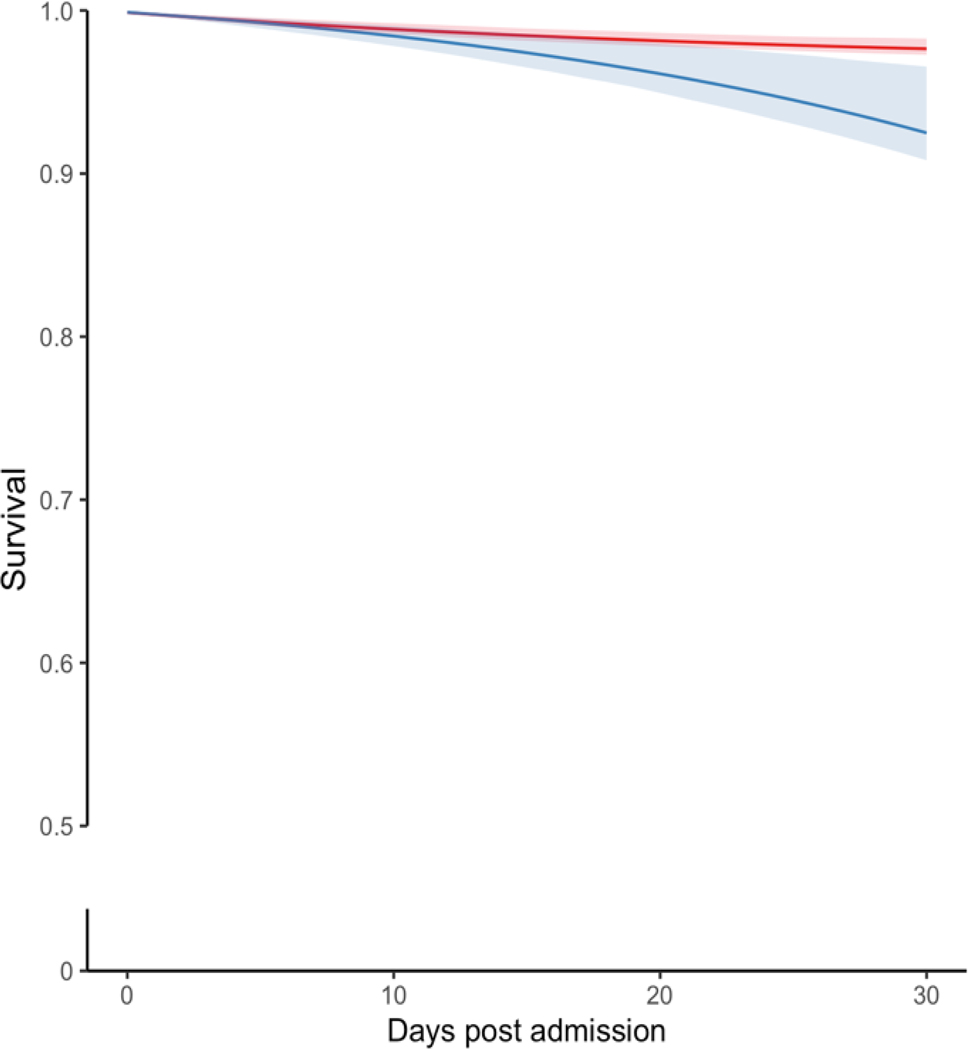
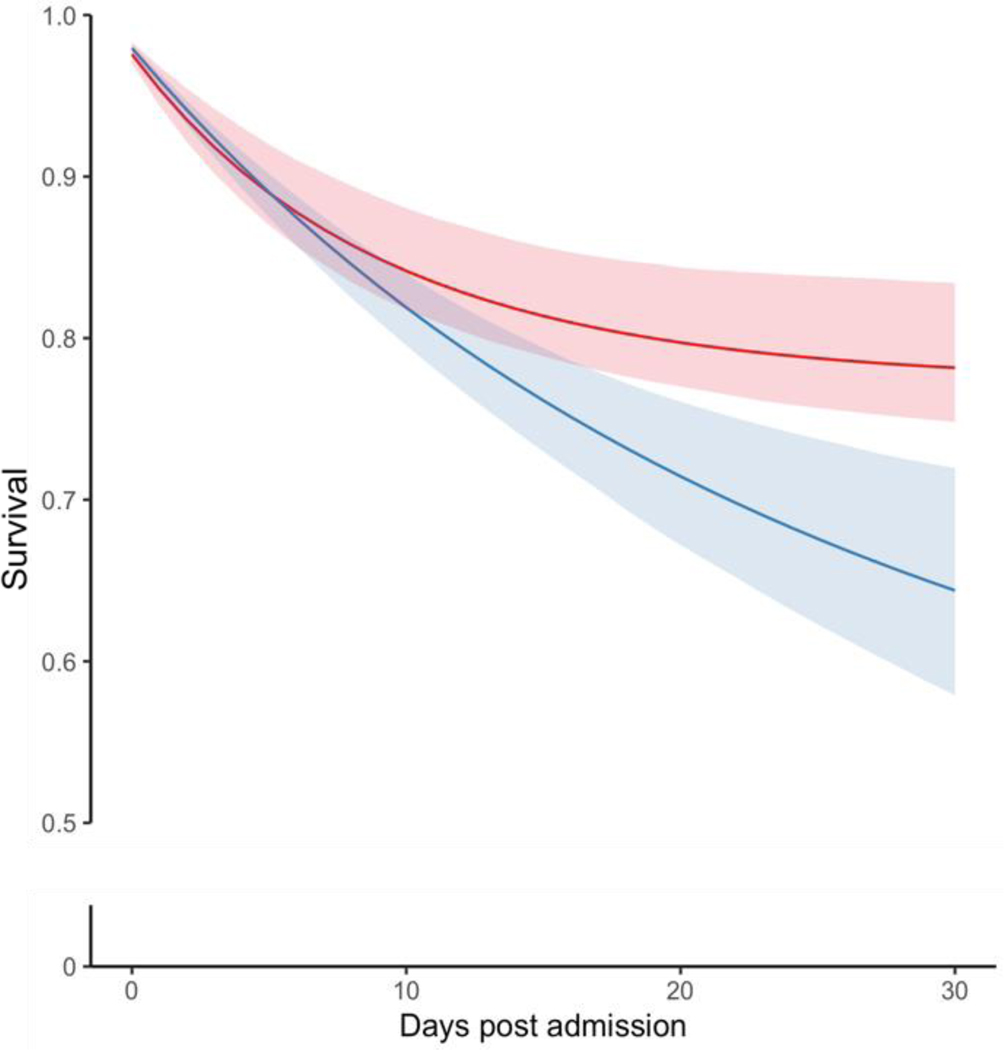
Results: The study sample included 151 patients who received antiseizure drugs and 3020 who did not. The crude 30-day mortality risks were 219 deaths per 1000 patients among epilepsy-specific antiseizure drugs initiators and 120 deaths per 1000 among noninitiators. After standardization, the estimated mortality was 251 (95% CI, 190-307) deaths per 1000 among initiators and 120 (95% CI, 86-144) deaths per 1000 among noninitiators, corresponding to a risk difference of 131 (95% CI, 65-200) excess deaths per 1000 patients. In the prespecified subgroup analyses, the risk difference was 52 (95% CI, 11-72) among patients with minor AIS and 138 (95% CI, 52-222) among moderate-to-severe AIS patients. Similarly, the risk differences were 86 (95% CI, 18-118) and 157 (95% CI, 57-219) among patients aged 65 to 74 years and ≥75 years, respectively.
Conclusions: There was a higher risk of 30-day mortality associated with initiating versus not initiating seizure prophylaxis within 7 days post-AIS. This study does not support the role of seizure prophylaxis in reducing 30-day poststroke mortality.
Keywords: anticonvulsants; ischemic stroke; neurology; seizures.
Figures
References
-
- Global Health Data Exchange 2017. Available At: Http://Ghdx.Healthdata.Org/Gbd-Results-Tool.
-
- Katan M, Luft A. Global Burden of Stroke. Semin Neurol. 2018;38:208–211 - PubMed
-
- Medicare Payment Advisory Commission (Medpac). March 2019 Report to the Congress: Medicare Payment Policy. Available At: Http://Medpac.Gov/Docs/Default-Source/Reports/Mar19_Medpac_Entirereport_.... 2019
MeSH terms
Grants and funding
- U19 AG062682/AG/NIA NIH HHS/United States
- R01 DK128150/DK/NIDDK NIH HHS/United States
- R01 AG063975/AG/NIA NIH HHS/United States
- U01 AG032984/AG/NIA NIH HHS/United States
- U24 NS100591/NS/NINDS NIH HHS/United States
- R01 NS104143/NS/NINDS NIH HHS/United States
- U24 NS107243/NS/NINDS NIH HHS/United States
- R01 AG062282/AG/NIA NIH HHS/United States
- R01 HD098421/HD/NICHD NIH HHS/United States
- R01 HD088393/HD/NICHD NIH HHS/United States
- R01 AG066793/AG/NIA NIH HHS/United States
- U01 AG076478/AG/NIA NIH HHS/United States
- R01 AG058063/AG/NIA NIH HHS/United States
- R01 DK107972/DK/NIDDK NIH HHS/United States
- T32 AG051108/AG/NIA NIH HHS/United States
- U01 AG068221/AG/NIA NIH HHS/United States
- P30 AG062421/AG/NIA NIH HHS/United States
- P01 AG036694/AG/NIA NIH HHS/United States
- U48DP006377/ACL/ACL HHS/United States
- R01 AG073410/AG/NIA NIH HHS/United States
- R01 AG048351/AG/NIA NIH HHS/United States
- U48 DP006377/DP/NCCDPHP CDC HHS/United States
- P01 AG032952/AG/NIA NIH HHS/United States
- P50 CA244433/CA/NCI NIH HHS/United States
- T32 MH017119/MH/NIMH NIH HHS/United States
