

Citicoline: pharmacological and clinical review, 2022 update
- PMID: 36544369
- PMCID: PMC10548480
- DOI: 10.33588/rn.75s05.2022311
Citicoline: pharmacological and clinical review, 2022 update
Abstract
This review is based on the previous one published in 2016 (Secades JJ. Citicoline: pharmacological and clinical review, 2016 update. Rev Neurol 2016; 63 (Supl 3): S1-S73), incorporating 176 new references, having all the information available in the same document to facilitate the access to the information in one document. This review is focused on the main indications of the drug, as acute stroke and its sequelae, including the cognitive impairment, and traumatic brain injury and its sequelae. There are retrieved the most important experimental and clinical data in both indications.
Title: Citicolina: revisión farmacológica y clínica, actualización 2022.
Esta revisión se basa en la publicada en 2016 –Secades JJ. Citicolina: revisión farmacológica y clínica, actualización 2016. Rev Neurol 2016; 63 (Supl 3): S1-S73–, e incorpora 176 nuevas referencias aparecidas desde entonces, con toda la información disponible para facilitar el acceso a toda la información en un único documento. La revisión se centra en las principales indicaciones del fármaco, como los accidentes cerebrovasculares agudos y sus secuelas, incluyendo el deterioro cognitivo, y los traumatismos craneoencefálicos y sus secuelas. Se recogen los principales aspectos experimentales y clínicos en estas indicaciones.
Conflict of interest statement
Conflicto de intereses: J.J.S. trabaja en el Departamento Médico de Ferrer.
Figures
Similar articles
-
Citicoline: pharmacological and clinical review, 2016 update.Rev Neurol. 2016 Dec 23;63(S03):S1-S73. Rev Neurol. 2016. PMID: 28417449 Review. English, Spanish.
-
Citicoline: pharmacological and clinical review, 2010 update.Rev Neurol. 2011 Mar 14;52 Suppl 2:S1-S62. Rev Neurol. 2011. PMID: 21432836 Review. English, Spanish.
-
Probably role of citicoline in stroke rehabilitation: review of the literature.Rev Neurol. 2012 Feb 1;54(3):173-9. Rev Neurol. 2012. PMID: 22278894 Review. English, Spanish.
-
Citicoline preclinical and clinical update 2009-2010.Stroke. 2011 Jan;42(1 Suppl):S36-9. doi: 10.1161/STROKEAHA.110.605568. Epub 2010 Dec 16. Stroke. 2011. PMID: 21164116 Review.
-
Efficacy of citicoline as an acute stroke treatment.Expert Opin Pharmacother. 2009 Apr;10(5):839-46. doi: 10.1517/17460440902835475. Expert Opin Pharmacother. 2009. PMID: 19351232
Cited by
-
Clinical Efficacy and Metabolomics Modifications Induced by Polyphenol Compound Supplementation in the Treatment of Residual Dizziness following Semont Maneuver in Benign Paroxysmal Positional Vertigo (BPPV) of the Posterior Semicircular Canal (PSC): Preliminary Results.Metabolites. 2024 Jan 25;14(2):86. doi: 10.3390/metabo14020086. Metabolites. 2024. PMID: 38392978 Free PMC article.
-
Successful treatment with guanfacine in a long-COVID case manifesting marked cognitive impairment.Neuropsychopharmacol Rep. 2024 Sep;44(3):585-590. doi: 10.1002/npr2.12466. Epub 2024 Jun 27. Neuropsychopharmacol Rep. 2024. PMID: 38934345 Free PMC article.
-
Exploring the Therapeutic Potential: Bioactive Molecules and Dietary Interventions in Multiple Sclerosis Management.Curr Issues Mol Biol. 2024 Jun 3;46(6):5595-5613. doi: 10.3390/cimb46060335. Curr Issues Mol Biol. 2024. PMID: 38921006 Free PMC article. Review.
-
Dopamine and Citicoline-Co-Loaded Solid Lipid Nanoparticles as Multifunctional Nanomedicines for Parkinson's Disease Treatment by Intranasal Administration.Pharmaceutics. 2024 Aug 7;16(8):1048. doi: 10.3390/pharmaceutics16081048. Pharmaceutics. 2024. PMID: 39204393 Free PMC article.
-
Real-life management of patients with mild cognitive impairment: an Italian survey.Neurol Sci. 2024 Sep;45(9):4279-4289. doi: 10.1007/s10072-024-07478-9. Epub 2024 Mar 25. Neurol Sci. 2024. PMID: 38528281 Free PMC article.
References
-
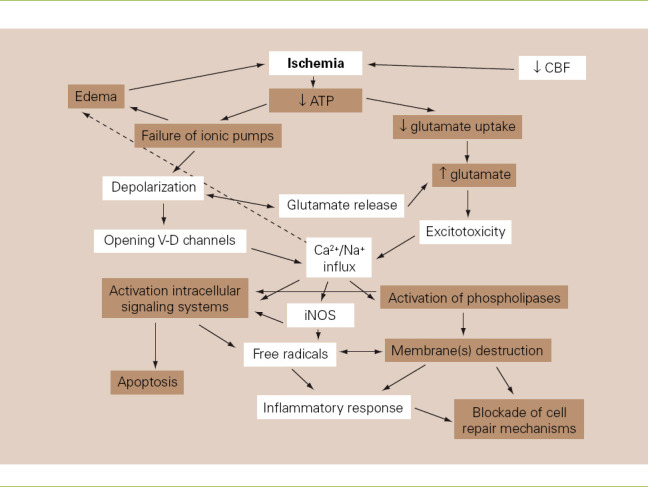
- Lozano R. La membrana neuronal:implicaciones terapéuticas. Boletín de Neurología. 1993;2:3–8.
-
- McMurray WC, Magee WL. Phospholipid metabolism. Ann Rev Biochem. 1972;41:129–61. - PubMed
-
- Nilsson B. CDP-choline:a short review. In: Tognon G, Garattini S, editors. Drug treatment and prevention in cerebrovascular disorders. Amsterdam: Elsevier/North Holland Biomedical Press; 1979. pp. 273–7.
-
- Kennedy EP, Weiss SB. The function of cytidine coenzymes in the biosynthesis of phospholipides. J Biol Chem. 1956;222:193–214. - PubMed
-
- McMaster CR. From yeast to humans - roles of the Kennedy pathway for phosphatidylcholine synthesis. FEBS Lett. 2018;592:1256–72. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
