

Added Value of the Sliding Sign on Right Down Decubitus CT for Determining Adjacent Organ Invasion in Patients with Advanced Gastric Cancer
- PMID: 36545416
- PMCID: PMC9748461
- DOI: 10.3348/jksr.2021.0166
Added Value of the Sliding Sign on Right Down Decubitus CT for Determining Adjacent Organ Invasion in Patients with Advanced Gastric Cancer
Abstract
Purpose: To investigate the added value of right down decubitus (RDD) CT when determining adjacent organ invasion in cases of advanced gastric cancer (AGC).
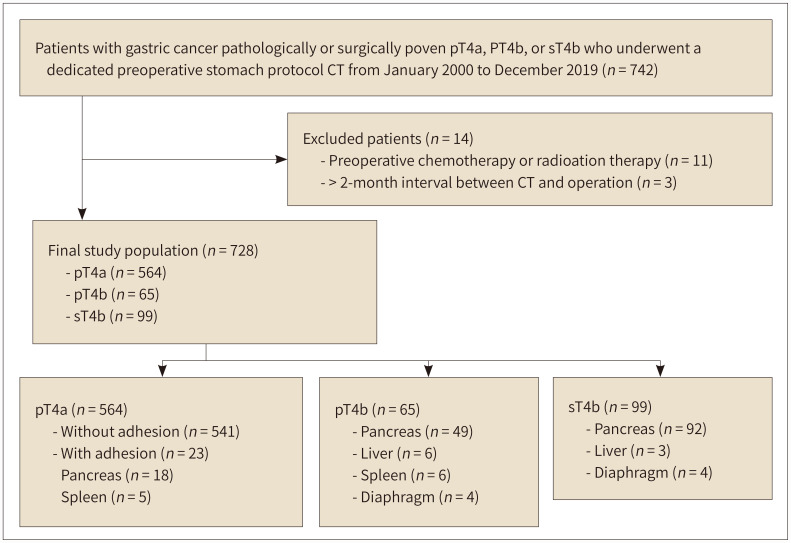
Materials and methods: A total of 728 patients with pathologically confirmed T4a (pT4a), surgically confirmed T4b (sT4b), or pathologically confirmed T4b (pT4b) AGCs who underwent dedicated stomach-protocol CT, including imaging of the left posterior oblique (LPO) and RDD positions, were included in this study. Two radiologists scored the T stage of AGCs using a 5-point scale on LPO CT with and without RDD CT at 2-week intervals and recorded the presence of "sliding sign" in the tumors and adjacent organs and compared its incidence of appearance.
Results: A total of 564 patients (77.4%) were diagnosed with pT4a, whereas 65 (8.9%) and 99 (13.6%) patients were diagnosed with pT4b and sT4b, respectively. When RDD CT was performed additionally, both reviewers deemed that the area under the curve (AUC) for differentiating T4b from T4a increased (p < 0.001). According to both reviewers, the AUC for differentiating T4b with pancreatic invasion from T4a increased in the subgroup analysis (p < 0.050). Interobserver agreement improved from fair to moderate (weighted kappa value, 0.296-0.444).
Conclusion: RDD CT provides additional value compared to LPO CT images alone for determining adjacent organ invasion in patients with AGC due to their increased AUC values and improved interobserver agreement.
목적: 진행성 위암의 인접 장기 침범을 결정함에 있어 우측와위 CT의 추가적 가치를 살펴보았다.
대상과 방법: 병리학적으로 입증된 T4a (p4a), 외과적 그리고 병리학적으로 입증된 T4b (sT4b, pT4b) 위암 환자 중 좌후사위 및 우측와위 자세가 포함된 프로토콜의 CT를 촬영한 환자 총 728명이 포함되었다. 2명의 영상의학과 전문의가 2주 간격으로 각각 우측와위 CT 없이, 우측와위 CT와 함께 좌후사위 CT를 분석하여 5점 척도를 사용하여 T 병기를 평가하고 종양과 인접 장기 사이의 “미끄러짐 징후”의 존재를 기록했다.
결과: 564명의 환자(77.4%)가 pT4a로 진단되었다. 65명(8.9%)과 99명(13.6%)의 환자가 각각 pT4b, sT4b로 진단되었다. 좌후사위 CT 단독 분석에 비하여 우측와위 CT가 추가되었을 때, T4b와 T4a를 구별하기 위한 곡선 아래 면적(area under the curve; 이하 AUC) 값이 두 검토자 모두에서 유의하게 증가했다(Ps < 0.001). 하위집단분석에서 T4a와 췌장을 침범한 T4b 위암을 구별하기 위한 AUC 값 역시 두 검토자 모두에서 증가했다(Ps < 0.050). 관찰자 간 일치도 역시 향상되었다(가중 카파 계수, 0.296–0.444).
결론: 진행위암에서 인접 장기 침범을 판단함에 있어, 우측와위 CT가 추가되었을 때 좌후사위 CT 단독 분석에 비해 더 높은 AUC 값과 관찰자 간 일치도를 보임으로써 추가적 가치가 있었다.
Keywords: Multidetector Computed Tomography; Neoplasm Invasiveness; Pancreas; Stomach Neoplasms; Task Performance and Analysis.
Copyrights © 2022 The Korean Society of Radiology.
Conflict of interest statement
Conflicts of Interest: The authors have no potential conflicts of interest to disclose.
Figures





References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
-
- Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005;55:74–108. - PubMed
-
- De Vita F, Giuliani F, Galizia G, Belli C, Aurilio G, Santabarbara G, et al. Neo-adjuvant and adjuvant chemotherapy of gastric cancer. Ann Oncol. 2007;18 Suppl 6:vi120–vi123. - PubMed
LinkOut - more resources
Full Text Sources
