

Very high-power short-duration ablation for pulmonary vein isolation utilizing a very-close protocol-the FAST AND FURIOUS PVI study
- PMID: 36546582
- PMCID: PMC10062369
- DOI: 10.1093/europace/euac243
Very high-power short-duration ablation for pulmonary vein isolation utilizing a very-close protocol-the FAST AND FURIOUS PVI study
Abstract
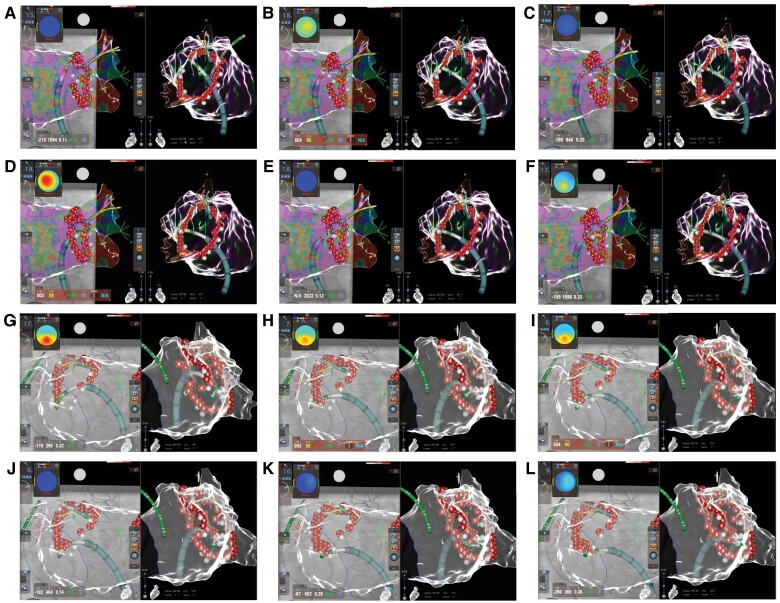
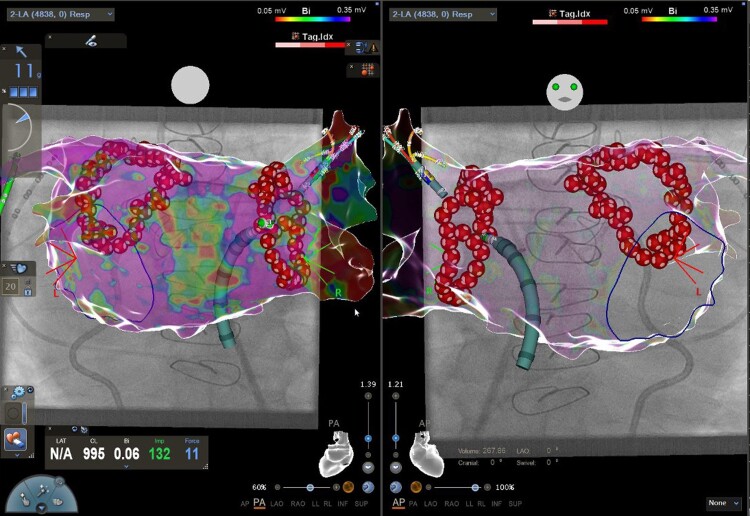
Aims: The very high-power short-duration (vHP-SD) radiofrequency (RF) ablation concept of atrial fibrillation (AF) treatment by pulmonary vein isolation (PVI) aims for safer, more effective, and faster procedures. Utilizing conventional ablation, the 'close protocol' has been verified. Since lesion formation of vHP-SD ablation creates wider but shallower lesions we adapted the close protocol to an individualized and tighter 'very-close protocol' of 3-4 mm of inter-lesion distance (ILD) at the anterior and 5-6 mm at the posterior aspect of the left atrium using vHP-SD only. Here, we evaluated the safety and efficacy of vHP-SD ablation for PVI utilizing a very-close protocol in comparison with standard ablation.
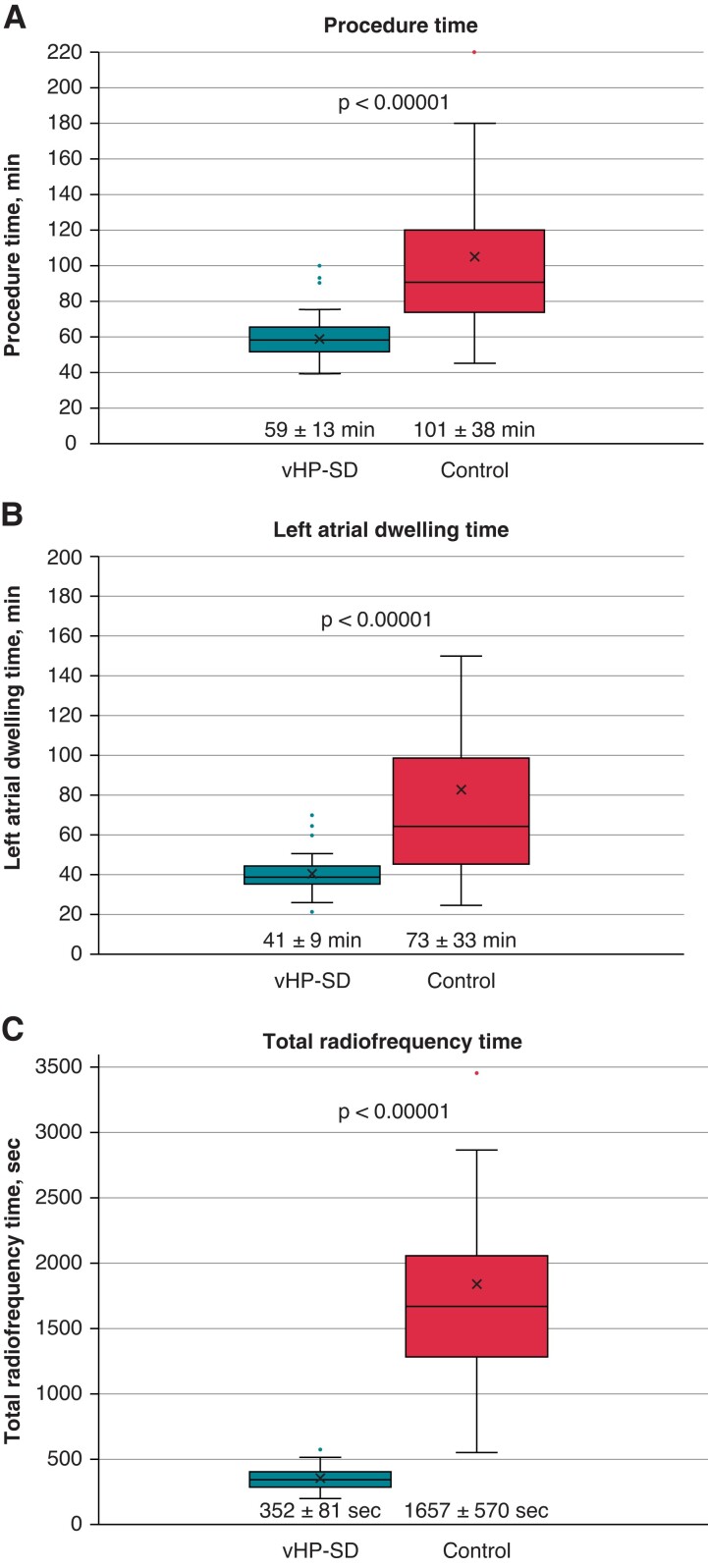
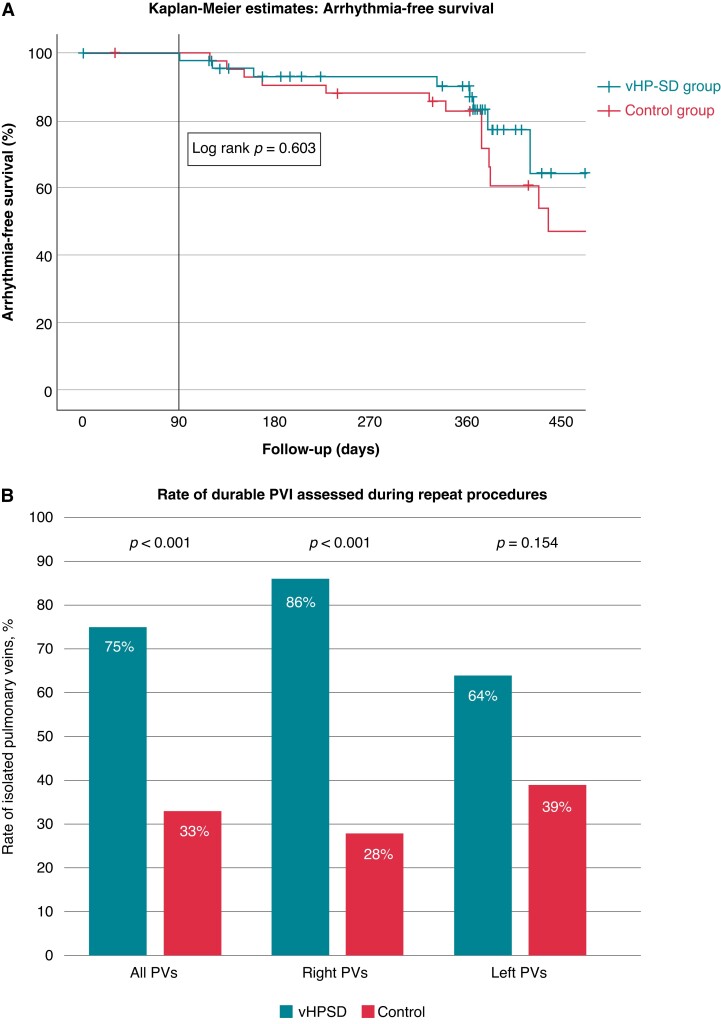
Methods and results: A total of 50 consecutive patients with symptomatic AF were treated with a very-close protocol utilizing vHP-SD (vHP-SD group). The data were compared with 50 consecutive patients treated by the ablation-index-guided strategy (control group). The mean RF time was 352 ± 81 s (vHP-SD) and 1657 ± 570 s (control, P < 0.0001), and the mean procedure duration was 59 ± 13 (vHP-SD) and 101 ± 38 (control, P < 0.0001). The first-pass isolation rate was 74% (vHP-SD) and 76% (control, P = 0.817). Severe adverse events were reported in 1 (2%, vHP-SD) and 3 (6%, control) patients (P = 0.307). A 12-month recurrence-free survival was 78% (vHP-SD) and 64% (control, P = 0.142). PVI durability assessed during redo-procedures was 75% (vHP-SD) vs. 33% (control, P < 0.001).
Conclusions: PVI solely utilizing vHP-SD via a very-close protocol provides safe and effective procedures with a high rate of first-pass isolations. The procedure duration and ablation time were remarkably low. A 12-month follow-up and PVI durability are promising.
Keywords: Acute efficacy; Atrial fibrillation; High-power short-duration; Pulmonary vein isolation; Radiofrequency.
© The Author(s) 2022. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: C.-H.H. received travel grants and research grants from Boston Scientific, Biosense Webster, and Cardiofocus, and Speaker’s Honoraria from Boston Scientific, Biosense Webster, and Cardiofocus. R.R.T. is a consultant of Boston Scientific, Biotronik, and Biosense Webster, and received Speaker’s Honoraria from Biosense Webster, Medtronic, Boston Scientific, and Abbot Medical. K.-H.K. reports grants and personal fees from Abbott Vascular, Medtronic, Biosense Webster outside submitted work. All other authors have no relevant disclosures. C.E. received travel grants and research grants by Boston Scientific, Biosense Webster, Medtronic, Abbott, and Speaker’s Honoraria from Boston Scientific, Biosense Webster Medtronic, and Abbott. All other authors none declared.
Figures
References
-
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist Cet al. . 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): the Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J 2020;42:373–498. - PubMed
-
- Kuck K-H, Brugada J, Fürnkranz A, Metzner A, Ouyang F, Chun KRJet al. . Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. New Engl J Med 2016;374:2235–45. - PubMed
-
- Hussein A, Das M, Chaturvedi V, Asfour IK, Daryanani N, Morgan Met al. . Prospective use of ablation index targets improves clinical outcomes following ablation for atrial fibrillation. J Cardiovasc Electrophysiol 2017;28:1037–47. - PubMed
-
- Hussein A, Das M, Riva S, Morgan M, Ronayne C, Sahni Aet al. . Use of ablation index-guided ablation results in high rates of durable pulmonary vein isolation and freedom from arrhythmia in persistent atrial fibrillation patients. Circ Arrhythm Electrophysiol 2018;11:e006576. - PubMed
-
- Kottmaier M, Popa M, Bourier F, Reents T, Cifuentes J, Semmler Vet al. . Safety and outcome of very high-power short-duration ablation using 70 W for pulmonary vein isolation in patients with paroxysmal atrial fibrillation. Ep Europace 2019;22:388–93. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
