

Sotorasib in KRAS p.G12C-Mutated Advanced Pancreatic Cancer
- PMID: 36546651
- PMCID: PMC10506456
- DOI: 10.1056/NEJMoa2208470
Sotorasib in KRAS p.G12C-Mutated Advanced Pancreatic Cancer
Abstract
Background: KRAS p.G12C mutation occurs in approximately 1 to 2% of pancreatic cancers. The safety and efficacy of sotorasib, a KRAS G12C inhibitor, in previously treated patients with KRAS p.G12C-mutated pancreatic cancer are unknown.
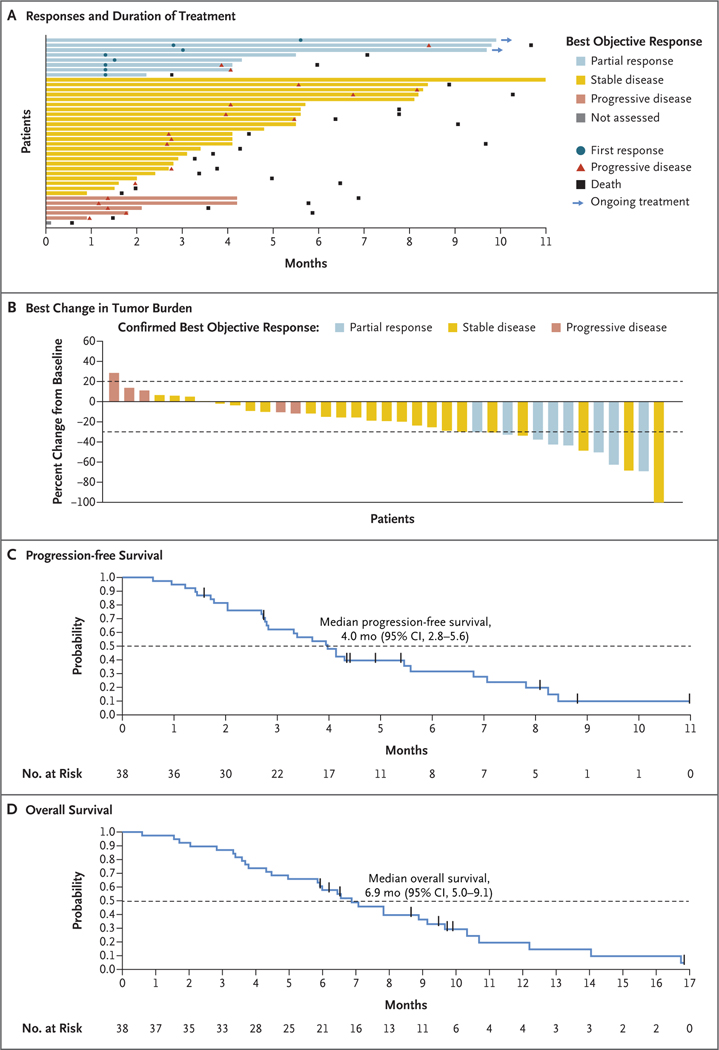
Methods: We conducted a single-group, phase 1-2 trial to assess the safety and efficacy of sotorasib treatment in patients with KRAS p.G12C-mutated pancreatic cancer who had received at least one previous systemic therapy. The primary objective of phase 1 was to assess safety and to identify the recommended dose for phase 2. In phase 2, patients received sotorasib at a dose of 960 mg orally once daily. The primary end point for phase 2 was a centrally confirmed objective response (defined as a complete or partial response). Efficacy end points were assessed in the pooled population from both phases and included objective response, duration of response, time to objective response, disease control (defined as an objective response or stable disease), progression-free survival, and overall survival. Safety was also assessed.
Results: The pooled population from phases 1 and 2 consisted of 38 patients, all of whom had metastatic disease at enrollment and had previously received chemotherapy. At baseline, patients had received a median of 2 lines (range, 1 to 8) of therapy previously. All 38 patients received sotorasib in the trial. A total of 8 patients had a centrally confirmed objective response (21%; 95% confidence interval [CI], 10 to 37). The median progression-free survival was 4.0 months (95% CI, 2.8 to 5.6), and the median overall survival was 6.9 months (95% CI, 5.0 to 9.1). Treatment-related adverse events of any grade were reported in 16 patients (42%); 6 patients (16%) had grade 3 adverse events. No treatment-related adverse events were fatal or led to treatment discontinuation.
Conclusions: Sotorasib showed anticancer activity and had an acceptable safety profile in patients with KRAS p.G12C-mutated advanced pancreatic cancer who had received previous treatment. (Funded by Amgen and others; CodeBreaK 100 ClinicalTrials.gov number, NCT03600883.).
Copyright © 2022 Massachusetts Medical Society.
Figures
Comment in
-
KRAS G12C inhibitors: also a new promising new targeted therapy in advanced pancreatic adenocarcinoma?Transl Cancer Res. 2023 Dec 31;12(12):3227-3232. doi: 10.21037/tcr-23-1629. Epub 2023 Nov 13. Transl Cancer Res. 2023. PMID: 38197074 Free PMC article. No abstract available.
References
-
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209–49. - PubMed
-
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011;3 64: 1817–25. - PubMed
-
- Wang-Gillam A, Hubner RA, Siveke JT, et al. NAPOLI-1 phase 3 study of liposomal irinotecan in metastatic pancreatic cancer: final overall survival analysis and characteristics of long-term survivors. Eur J Cancer 2019; 108: 78–87. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous