

Sex-related differences in left ventricular assist device utilization and outcomes: results from the PCHF-VAD registry
- PMID: 36547014
- PMCID: PMC10053365
- DOI: 10.1002/ehf2.14261
Sex-related differences in left ventricular assist device utilization and outcomes: results from the PCHF-VAD registry
Abstract
Aims: Data on sex and left ventricular assist device (LVAD) utilization and outcomes have been conflicting and mostly confined to US studies incorporating older devices. This study aimed to investigate sex-related differences in LVAD utilization and outcomes in a contemporary European LVAD cohort.
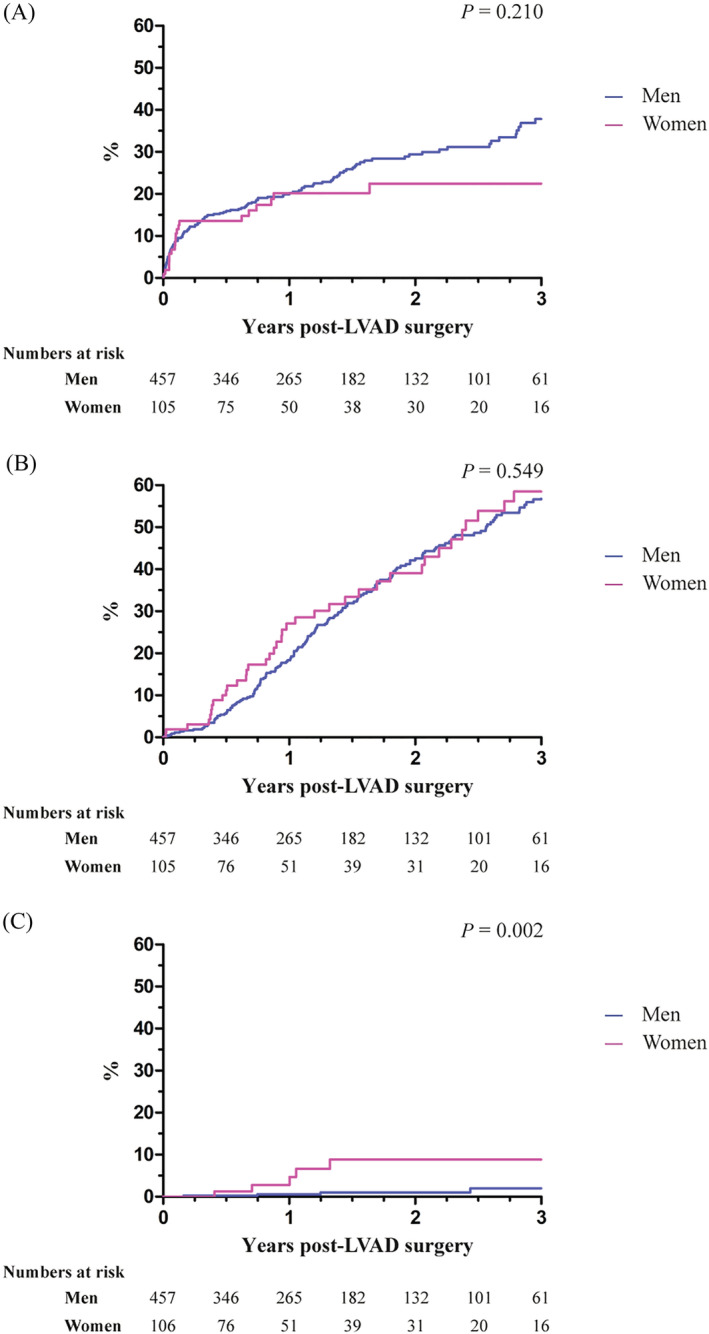
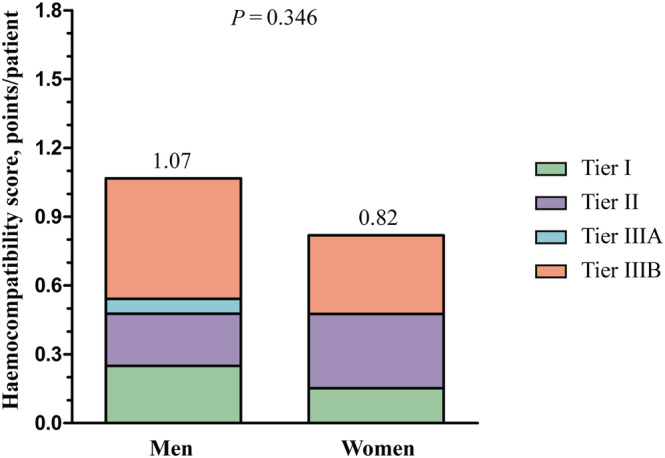
Methods and results: This analysis is part of the multicentre PCHF-VAD registry studying continuous-flow LVAD patients. The primary outcome was all-cause mortality. Secondary outcomes included ventricular arrhythmias, right ventricular failure, bleeding, thromboembolism, and the haemocompatibility score. Multivariable Cox regression models were used to assess associations between sex and outcomes. Overall, 457 men (81%) and 105 women (19%) were analysed. At LVAD implant, women were more often in Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) profile 1 or 2 (55% vs. 41%, P = 0.009) and more often required temporary mechanical circulatory support (39% vs. 23%, P = 0.001). Mean age was comparable (52.1 vs. 53.4 years, P = 0.33), and median follow-up duration was 344 [range 147-823] days for women and 435 [range 190-816] days for men (P = 0.40). No significant sex-related differences were found in all-cause mortality (hazard ratio [HR] 0.79 for female vs. male sex, 95% confidence interval [CI] [0.50-1.27]). Female LVAD patients had a lower risk of ventricular arrhythmias (HR 0.56, 95% CI [0.33-0.95]) but more often experienced right ventricular failure. No significant sex-related differences were found in other outcomes.
Conclusions: In this contemporary European cohort of LVAD patients, far fewer women than men underwent LVAD implantation despite similar clinical outcomes. This is important as the proportion of female LVAD patients (19%) was lower than the proportion of females with advanced HF as reported in previous studies, suggesting underutilization. Also, female patients were remarkably more often in INTERMACS profile 1 or 2, suggesting later referral for LVAD therapy. Additional research in female patients is warranted.
Keywords: Advanced heart failure; Left ventricular assist device; Sex; Survival; Utilization.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
N.J. reports personal fees and non‐financial support from Servier, personal fees from Teva Pharmaceutical Industries, Krka, Sanofi Genzyme, Boehringer Ingelheim, and Bayer, and non‐financial support from Abbott, outside the submitted work. A.C.P. reports personal fees from Novartis, Bayer, Vifor, and AstraZeneca, outside the submitted work. I.P. reports grants and personal fees from Boehringer Ingelheim, personal fees from Teva Pharmaceutical Industries, Servier, Krka, and Corvia, and personal fees and non‐financial support from Novartis, Pfizer, Bayer, Sandoz, Abbott, and Sanofi Aventis, outside the submitted work. A.J.F. reports personal fees from Alnylam, Bayer, Boehringer Ingelheim, Fresenius, Imedos Systems, Medtronic, MSD, Mundipharma, Pierre Fabre, Pfizer, Roche, Vifor, and ZOLL, and grants and personal fees from AstraZeneca and Novartis, outside the submitted work. L.H.L. reports personal fees from Merck, Bayer, Pharmacosmos, Abbott, Medscape, Myokardia, Sanofi, Lexicon, and Radcliffe Cardiology, grants and personal fees from Vifor‐Fresenius, AstraZeneca, Boehringer Ingelheim, and Novartis, and grants from Boston Scientific, outside the submitted work. D.M. reports personal fees from Boehringer Ingelheim, Bayer, Pfizer, Novartis, AstraZeneca, Novo Nordisk, Teva, and Servier, outside the submitted work. F.R. has not received personal payments by pharmaceutical companies or device manufacturers in the last 3 years (remuneration for the time spent in activities, such as participation as steering committee member of clinical trials and member of the Pfizer Research Award selection committee in Switzerland, were made directly to the University of Zurich). The Department of Cardiology (University Hospital of Zurich/University of Zurich) reports research, educational, and/or travel grants from Abbott, Amgen, AstraZeneca, Bayer, Berlin Heart, B. Braun, Biosense Webster, Biosensors Europe AG, Biotronik, BMS, Boehringer Ingelheim, Boston Scientific, Bracco, Cardinal Health Switzerland, Corteria, Daiichi, Diatools AG, Edwards Lifesciences, Guidant Europe NV (BS), Hamilton Health Sciences, Kaneka Corporation, Kantar, Labormedizinisches Zentrum, Medtronic, MSD, Mundipharma Medical Company, Novartis, Novo Nordisk, Orion, Pfizer, Quintiles Switzerland Sarl, Sahajanand IN, Sanofi, Sarstedt AG, Servier, SIS Medical, SSS International Clinical Research, Terumo Deutschland, Trama Solutions, V‐Wave, Vascular Medical, Vifor, Wissens Plus, and ZOLL. The research and educational grants do not impact on F.R.'s personal remuneration. M.C. reports grants and personal fees from Novartis, grants from Abbott, personalfees from GE Healthcare, Bayer, Boehringer Ingelheim, AstraZeneca, Teva Pharmaceutical Industries, Sanofi, and LivaNova, non‐financial support from Corvia, and personal fees and non‐financial support from Pfizer, outside the submitted work. J.J.B. reports personal fees from Abbott, outside the submitted work. All other authors have no conflict of interest to disclose.
Figures
References
-
- Lloyd‐Jones DM, Larson MG, Leip EP, Beiser A, D'Agostino RB, Kannel WB, Murabito JM, Vasan RS, Benjamin EJ, Levy D, Framingham Heart S. Lifetime risk for developing congestive heart failure: the Framingham Heart Study. Circulation. 2002; 106: 3068–3072. - PubMed
-
- He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK. Risk factors for congestive heart failure in US men and women: NHANES I epidemiologic follow‐up study. Arch Intern Med. 2001; 161: 996–1002. - PubMed
-
- Masoudi FA, Havranek EP, Smith G, Fish RH, Steiner JF, Ordin DL, Krumholz HM. Gender, age, and heart failure with preserved left ventricular systolic function. J Am Coll Cardiol. 2003; 41: 217–223. - PubMed
-
- Alehagen U, Ericsson A, Dahlström U. Are there any significant differences between females and males in the management of heart failure? Gender aspects of an elderly population with symptoms associated with heart failure. J Card Fail. 2009; 15: 501–507. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
