

Developing Artificial Intelligence Models for Extracting Oncologic Outcomes from Japanese Electronic Health Records
- PMID: 36547809
- PMCID: PMC9988800
- DOI: 10.1007/s12325-022-02397-7
Developing Artificial Intelligence Models for Extracting Oncologic Outcomes from Japanese Electronic Health Records
Abstract
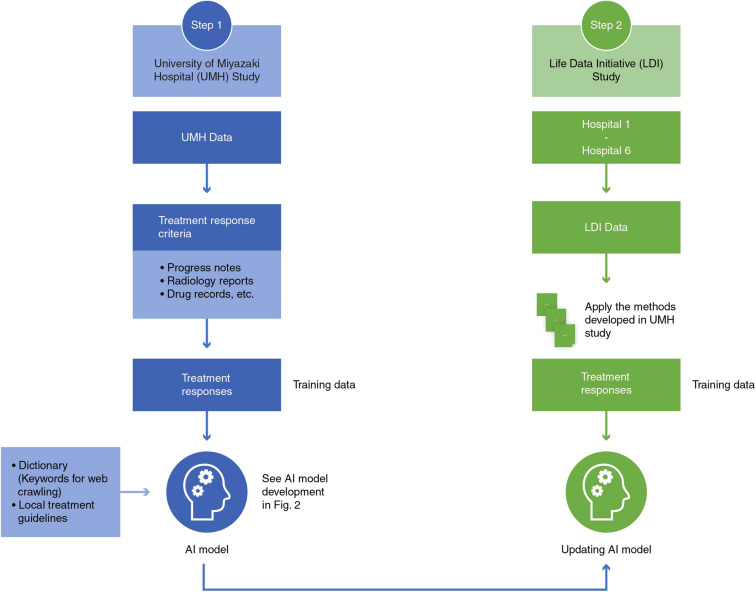
Introduction: A framework that extracts oncological outcomes from large-scale databases using artificial intelligence (AI) is not well established. Thus, we aimed to develop AI models to extract outcomes in patients with lung cancer using unstructured text data from electronic health records of multiple hospitals.
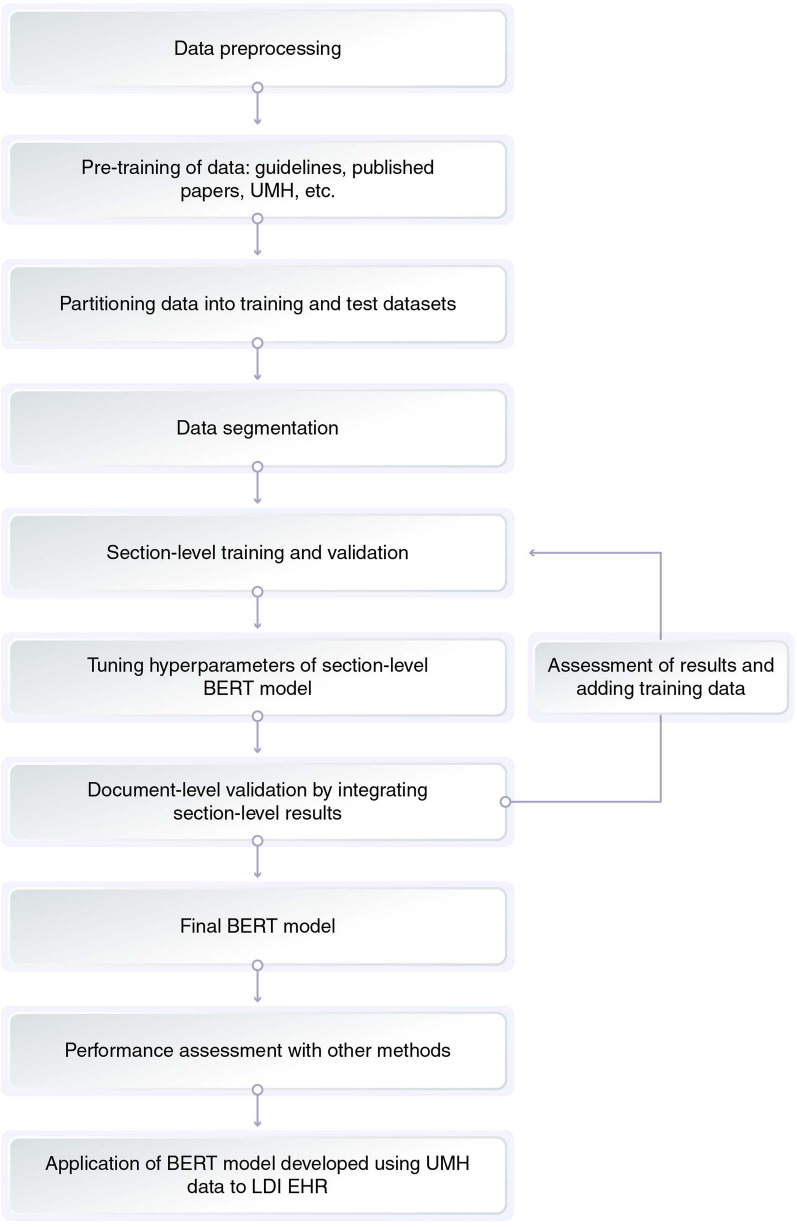
Methods: We constructed AI models (Bidirectional Encoder Representations from Transformers [BERT], Naïve Bayes, and Longformer) for tumor evaluation using the University of Miyazaki Hospital (UMH) database. This data included both structured and unstructured data from progress notes, radiology reports, and discharge summaries. The BERT model was applied to the Life Data Initiative (LDI) data set of six hospitals. Study outcomes included the performance of AI models and time to progression of disease (TTP) for each line of treatment based on the treatment response extracted by AI models.
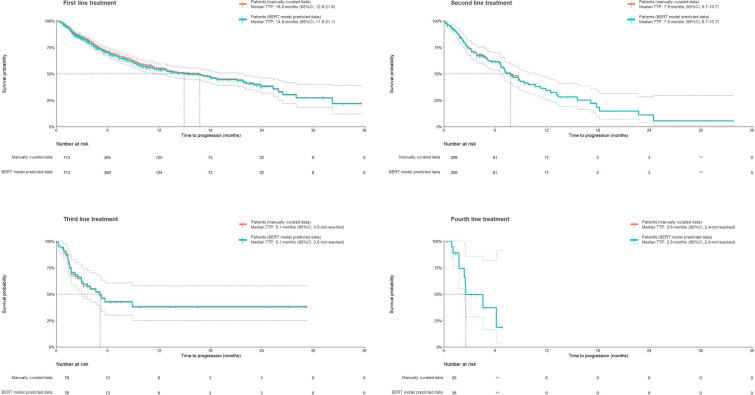
Results: For the UMH data set, the BERT model exhibited higher precision accuracy compared to the Naïve Bayes or the Longformer models, respectively (precision [0.42 vs. 0.47 or 0.22], recall [0.63 vs. 0.46 or 0.33] and F1 scores [0.50 vs. 0.46 or 0.27]). When this BERT model was applied to LDI data, prediction accuracy remained quite similar. The Kaplan-Meier plots of TTP (months) showed similar trends for the first (median 14.9 [95% confidence interval 11.5, 21.1] and 16.8 [12.6, 21.8]), the second (7.8 [6.7, 10.7] and 7.8 [6.7, 10.7]), and the later lines of treatment for the predicted data by the BERT model and the manually curated data.
Conclusion: We developed AI models to extract treatment responses in patients with lung cancer using a large EHR database; however, the model requires further improvement.
Keywords: Artificial intelligence; BERT; Electronic health records database; Lung cancer; Real-world data; Retrospective study.
Plain language summary
The use of artificial intelligence (AI) to derive health outcomes from large electronic health records is not well established. Thus, we built three different AI models: Bidirectional Encoder Representations from Transformers (BERT), Naïve Bayes, and Longformer to serve this purpose. Initially, we developed these models based on data from the University of Miyazaki Hospital (UMH) and later improved them using the Life Data Initiative (LDI) data set of six hospitals. The performance of the BERT model was better than the other two, and it showed similar results when it was applied to the LDI data set. The Kaplan–Meier plots of time to progression of disease for the predicted data by the BERT model showed similar trends to those for the manually curated data. In summary, we developed an AI model to extract health outcomes using a large electronic health database in this study; however, the performance of the AI model could be improved using more training data.
© 2022. The Author(s).
Figures
References
-
- Tayefi M, Ngo P, Chomutare T, et al. Challenges and opportunities beyond structured data in analysis of electronic health records. Wiley Interdiscip Rev Comput Stat. 2021;13(6):e1549. doi: 10.1002/wics.1549. - DOI
-
- Dalianis H. Clinical text mining: secondary use of electronic patient records. Cham: Springer Nature; 2018. 10.1007/978-3-319-78503-5.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
