

Association of SARS-CoV-2 Spike Protein Antibody Vaccine Response With Infection Severity in Patients With Cancer: A National COVID Cancer Cross-sectional Evaluation
- PMID: 36547970
- PMCID: PMC9936347
- DOI: 10.1001/jamaoncol.2022.5974
Association of SARS-CoV-2 Spike Protein Antibody Vaccine Response With Infection Severity in Patients With Cancer: A National COVID Cancer Cross-sectional Evaluation
Abstract
Importance: Accurate identification of patient groups with the lowest level of protection following COVID-19 vaccination is important to better target resources and interventions for the most vulnerable populations. It is not known whether SARS-CoV-2 antibody testing has clinical utility for high-risk groups, such as people with cancer.
Objective: To evaluate whether spike protein antibody vaccine response (COV-S) following COVID-19 vaccination is associated with the risk of SARS-CoV-2 breakthrough infection or hospitalization among patients with cancer.
Design, setting, and participants: This was a population-based cross-sectional study of patients with cancer from the UK as part of the National COVID Cancer Antibody Survey. Adults with a known or reported cancer diagnosis who had completed their primary SARS-CoV-2 vaccination schedule were included. This analysis ran from September 1, 2021, to March 4, 2022, a period covering the expansion of the UK's third-dose vaccination booster program.
Interventions: Anti-SARS-CoV-2 COV-S antibody test (Elecsys; Roche).
Main outcomes and measures: Odds of SARS-CoV-2 breakthrough infection and COVID-19 hospitalization.
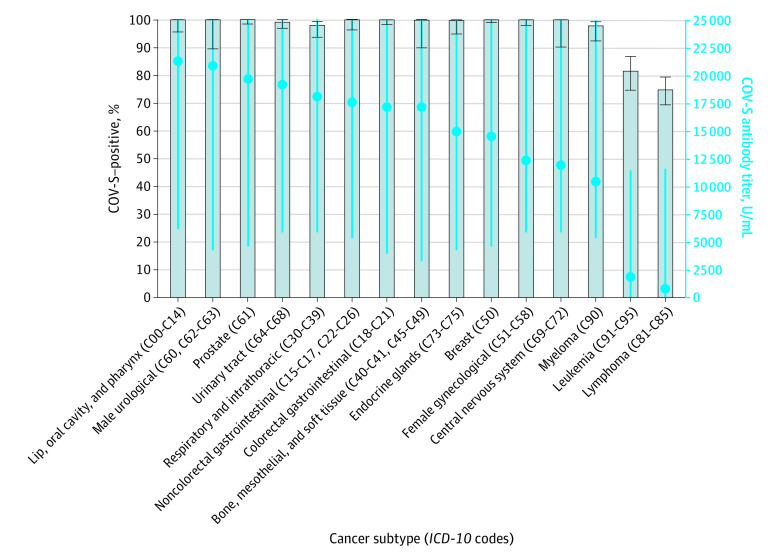
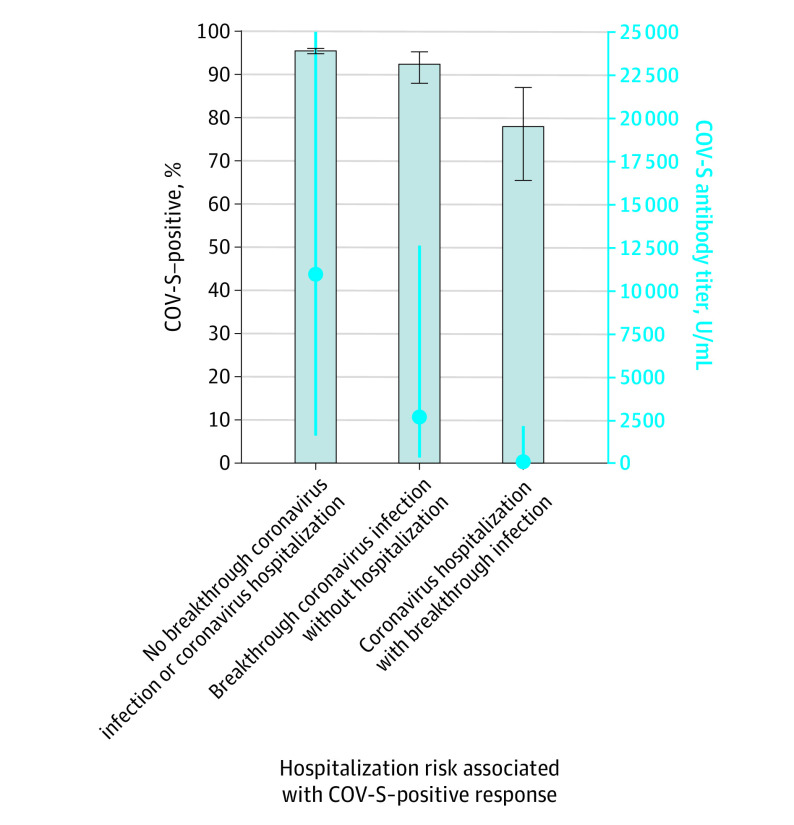
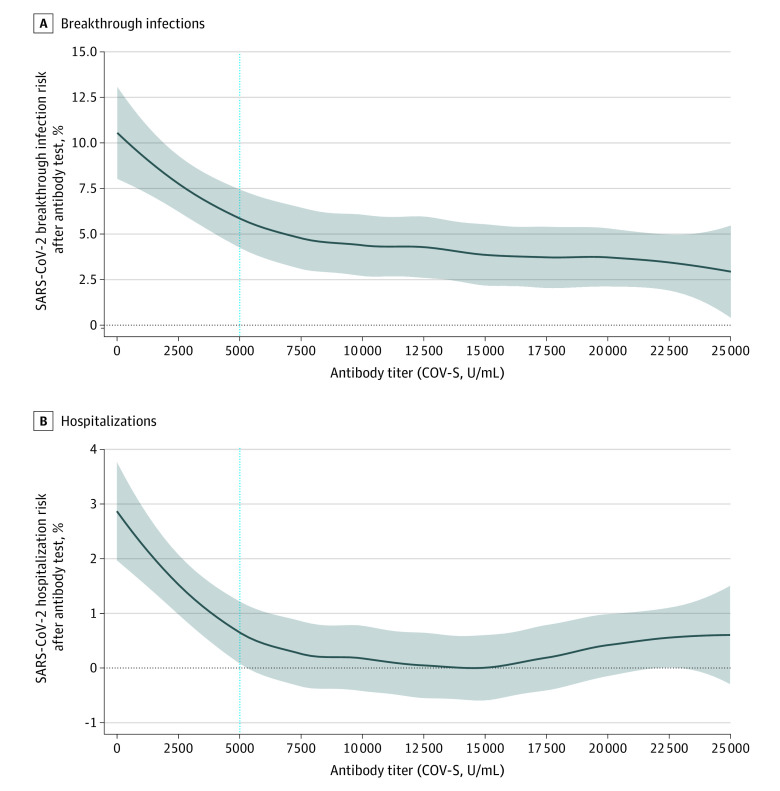
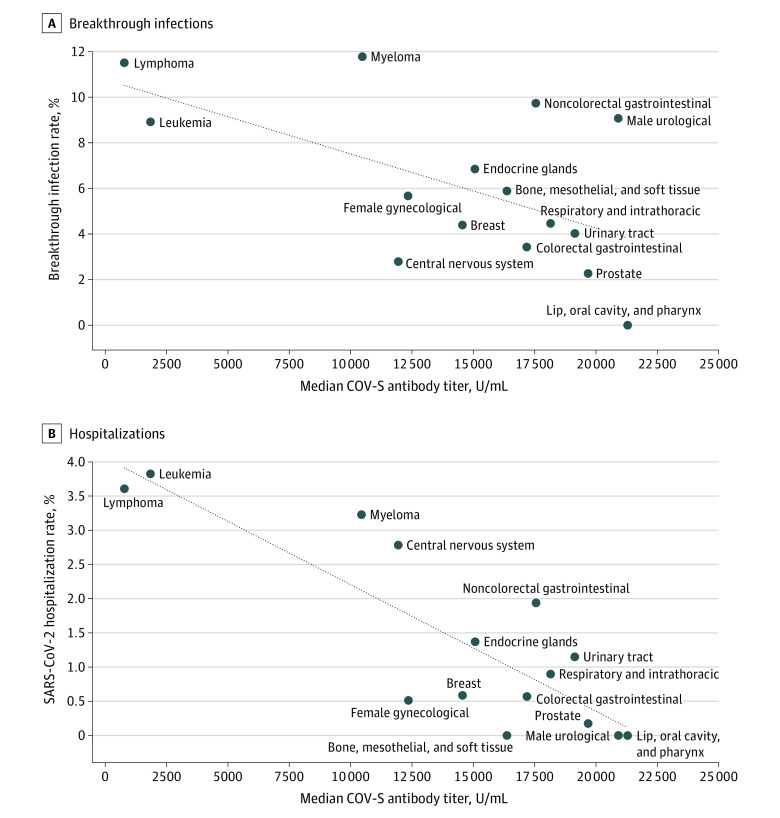
Results: The evaluation comprised 4249 antibody test results from 3555 patients with cancer and 294 230 test results from 225 272 individuals in the noncancer population. The overall cohort of 228 827 individuals (patients with cancer and the noncancer population) comprised 298 479 antibody tests. The median age of the cohort was in the age band of 40 and 49 years and included 182 741 test results (61.22%) from women and 115 737 (38.78%) from men. There were 279 721 tests (93.72%) taken by individuals identifying as White or White British. Patients with cancer were more likely to have undetectable anti-S antibody responses than the general population (199 of 4249 test results [4.68%] vs 376 of 294 230 [0.13%]; P < .001). Patients with leukemia or lymphoma had the lowest antibody titers. In the cancer cohort, following multivariable correction, patients who had an undetectable antibody response were at much greater risk for SARS-CoV-2 breakthrough infection (odds ratio [OR], 3.05; 95% CI, 1.96-4.72; P < .001) and SARS-CoV-2-related hospitalization (OR, 6.48; 95% CI, 3.31-12.67; P < .001) than individuals who had a positive antibody response.
Conclusions and relevance: The findings of this cross-sectional study suggest that COV-S antibody testing allows the identification of patients with cancer who have the lowest level of antibody-derived protection from COVID-19. This study supports larger evaluations of SARS-CoV-2 antibody testing. Prevention of SARS-CoV-2 transmission to patients with cancer should be prioritized to minimize impact on cancer treatments and maximize quality of life for individuals with cancer during the ongoing pandemic.
Conflict of interest statement
Figures
Comment in
-
Variability in COVID-19 Vaccine Response Among People With Cancer: What Health Care Strategy Best Protects the Vulnerable?JAMA Oncol. 2023 Feb 1;9(2):177-179. doi: 10.1001/jamaoncol.2022.5874. JAMA Oncol. 2023. PMID: 36547943 No abstract available.
-
Association of SARS-CoV-2 Antibody Level With Risk of Infection or Hospitalization.JAMA Oncol. 2023 Jun 1;9(6):870-871. doi: 10.1001/jamaoncol.2023.0775. JAMA Oncol. 2023. PMID: 37103923 No abstract available.
References
-
- Becerril-Gaitan A, Vaca-Cartagena BF, Ferrigno AS, et al. . Immunogenicity and risk of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection after coronavirus disease 2019 (COVID-19) vaccination in patients with cancer: a systematic review and meta-analysis. Eur J Cancer. 2022;160:243-260. doi:10.1016/j.ejca.2021.10.014 - DOI - PMC - PubMed
-
- Gounant V, Ferré VM, Soussi G, et al. . Efficacy of severe acute respiratory syndrome coronavirus-2 vaccine in patients with thoracic cancer: a prospective study supporting a third dose in patients with minimal serologic response after two vaccine doses. J Thorac Oncol. 2022;17(2):239-251. doi:10.1016/j.jtho.2021.10.015 - DOI - PMC - PubMed
-
- Fendler A, Au L, Shepherd STC, et al. ; Crick COVID-19 Consortium; CAPTURE Consortium . Functional antibody and T cell immunity following SARS-CoV-2 infection, including by variants of concern, in patients with cancer: the CAPTURE study. Nat Cancer. 2021;2(12):1321-1337. doi:10.1038/s43018-021-00275-9 - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
