

Malignancy risk in kidney transplant recipients exposed to immunosuppression pre-transplant for the treatment of glomerulonephritis
- PMID: 36549661
- PMCID: PMC10468752
- DOI: 10.1093/ndt/gfac337
Malignancy risk in kidney transplant recipients exposed to immunosuppression pre-transplant for the treatment of glomerulonephritis
Abstract
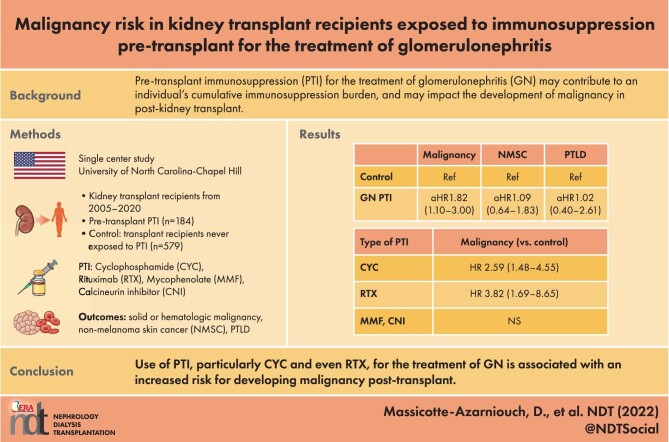
Background: Kidney transplant patients with glomerulonephritis (GN) as their native disease may receive significant amounts of pre-transplant immunosuppression (PTI), which could increase the risk for development of malignancy post-transplant.
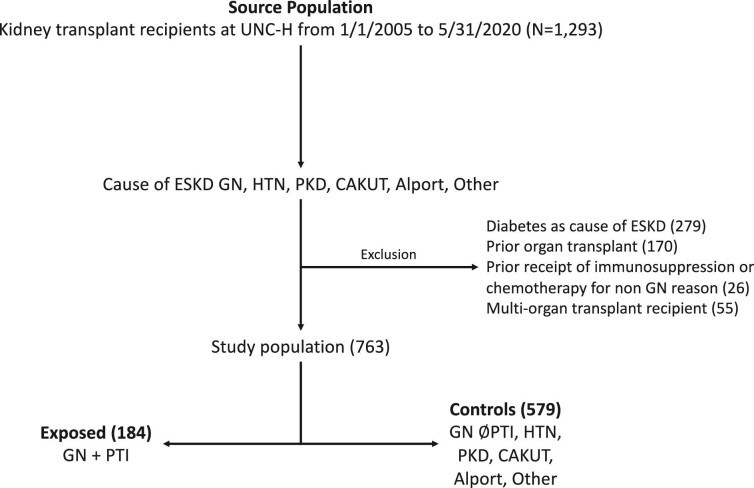
Methods: We conducted a single-center, retrospective study of kidney transplant recipients from January 2005 until May 2020. Patients with GN as their native kidney disease who received PTI for treatment of GN (n = 184) were compared with a control cohort (n = 579) of non-diabetic, non-PTI-receiving kidney transplant patients. We calculated hazard ratios (HR) with 95% confidence intervals (95% CI) for outcomes of first occurrence of solid or hematologic malignancy, non-melanoma skin cancer (NMSC) and post-transplant lymphoproliferative disorder (PTLD).
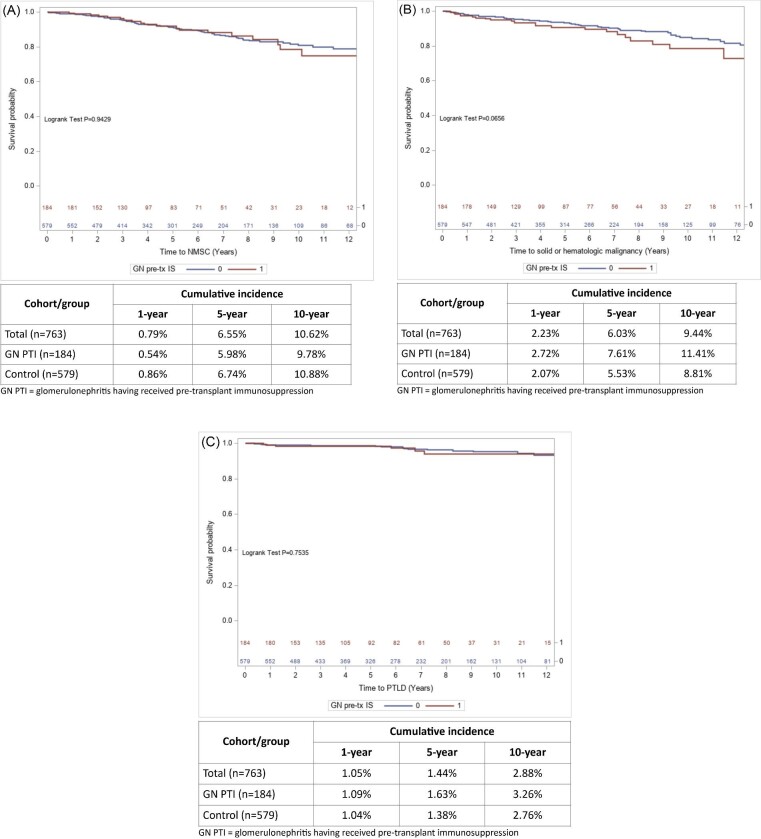
Results: Over a median follow-up of 5.7 years, PTI for GN was associated with significantly increased risk for malignancy compared with controls [13.0% vs 9.7%, respectively; adjusted HR 1.82 (95% CI 1.10-3.00)], but not for NMSC [10.3% vs 11.4%, respectively; adjusted HR 1.09 (95% CI 0.64-1.83)] or PTLD [3.3% vs 3.1%, respectively; adjusted HR 1.02 (95% CI 0.40-2.61)]. The risk for malignancy was significantly increased in those who received cyclophosphamide [HR 2.59 (95% CI 1.48-4.55)] or rituximab [HR 3.82 (95% CI 1.69-8.65)] pre-transplant, and particularly in those who received both cyclophosphamide and rituximab, but not for calcineurin inhibitors or mycophenolate.
Conclusion: The use of PTI for treatment of GN, especially cyclophosphamide or even with rituximab, is associated with increased risk for development of solid or hematologic malignancy post-transplant. These data highlight potential risks with treatment of GN and underscore the importance of post-transplant malignancy surveillance in this patient population.
Keywords: glomerulonephritis; immunosuppression; kidney transplant; malignancy; non-melanomatous skin cancer.
© The Author(s) 2022. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
V.K.D. reports consultancy agreements with Forma Therapeutics and Novartis; honoraria from UpToDate; and serving in an advisory role for Travere, Merck and Bayer. R.J.F. reports serving on an advisory board for Vertex Pharmaceuticals. M.K.S. reports honoraria from Calliditas, Elsevier, Chemocentryx and Travere therapeutics.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
