

Dupilumab increases aspirin tolerance in NSAID-exacerbated respiratory disease
- PMID: 36549708
- PMCID: PMC10017890
- DOI: 10.1183/13993003.01335-2022
Dupilumab increases aspirin tolerance in NSAID-exacerbated respiratory disease
Abstract
Background: Nonsteroidal anti-inflammatory drug (NSAID)-exacerbated respiratory disease (N-ERD) comprises the triad of chronic rhinosinusitis with nasal polyps, asthma and intolerance to NSAIDs. Dupilumab treatment, targeting the interleukin-4 (IL-4) receptor α, significantly reduces polyp burden as well as asthma symptoms. Here we aimed to investigate the effect of dupilumab on aspirin intolerance, burden of disease and nasal cytokine profiles in patients with N-ERD.
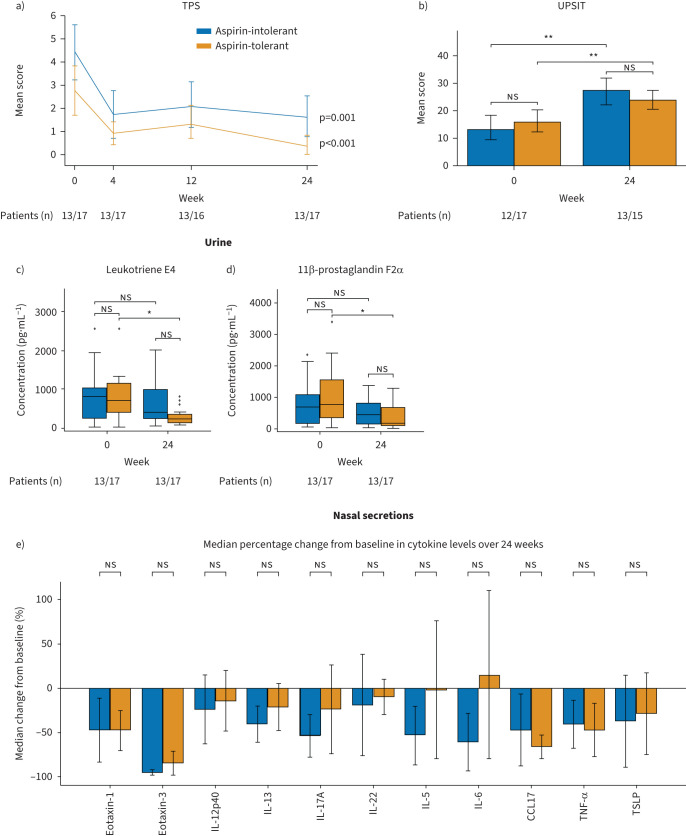
Methods: In this open-label trial, adult patients with confirmed N-ERD were treated with dupilumab for 6 months. Clinical parameters (e.g. total polyp scores, quality of life questionnaires, smell test, spirometry), oral aspirin provocation testing and blood, nasal and urine sampling were monitored at regular intervals for up to 6 months after starting dupilumab therapy.
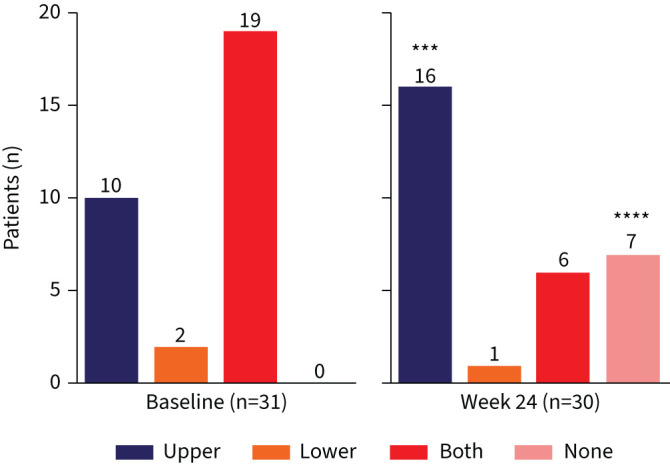
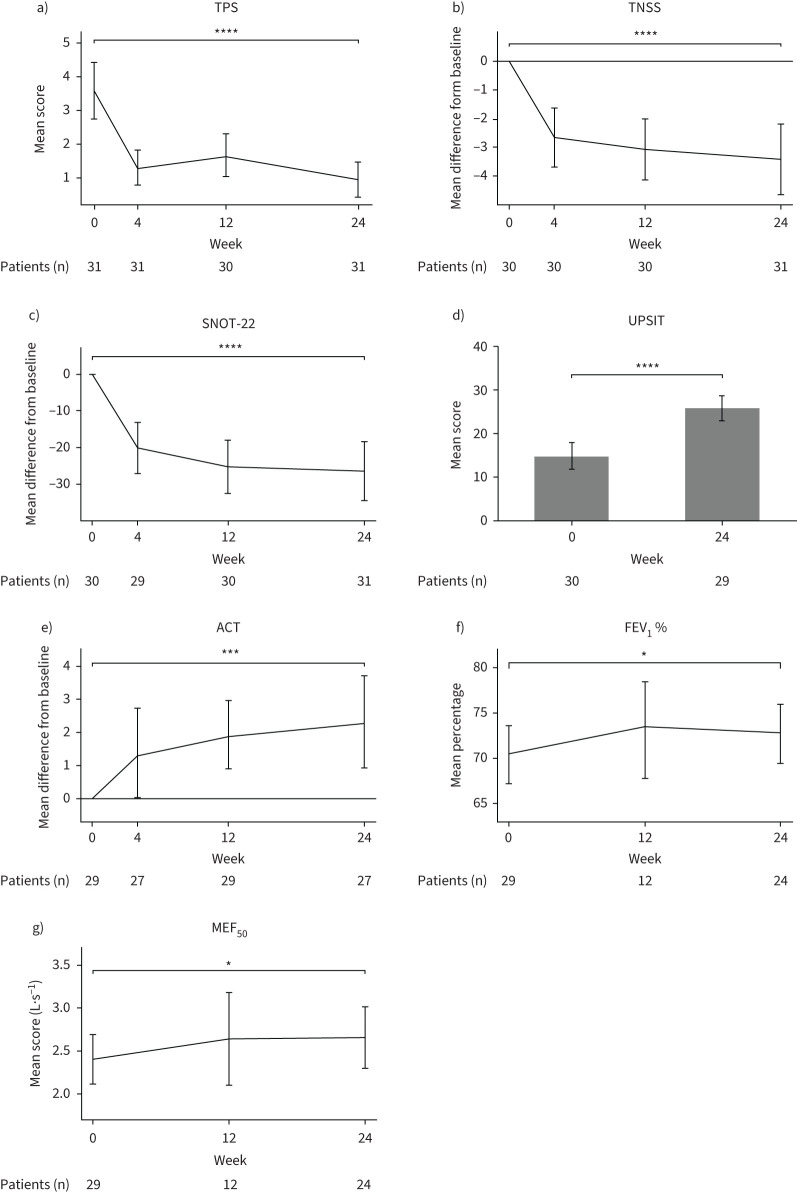
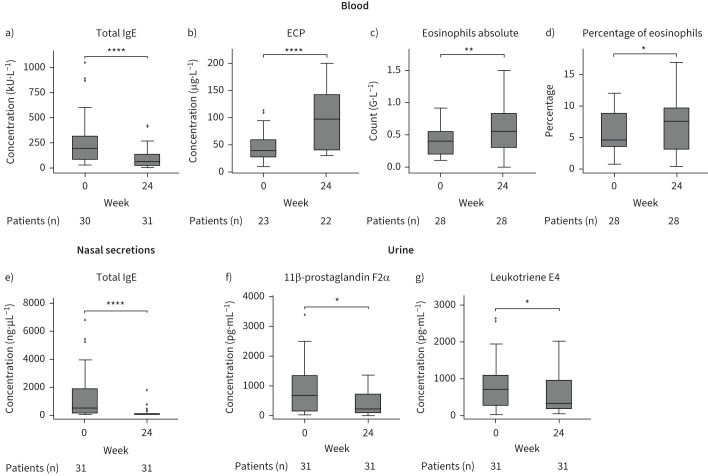
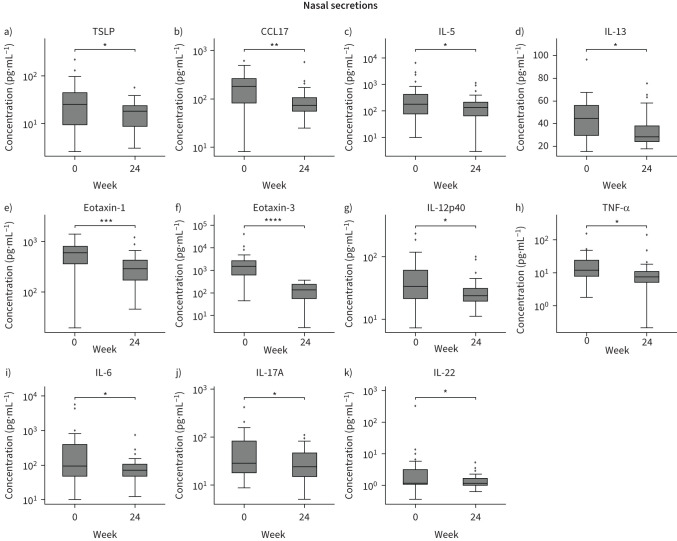
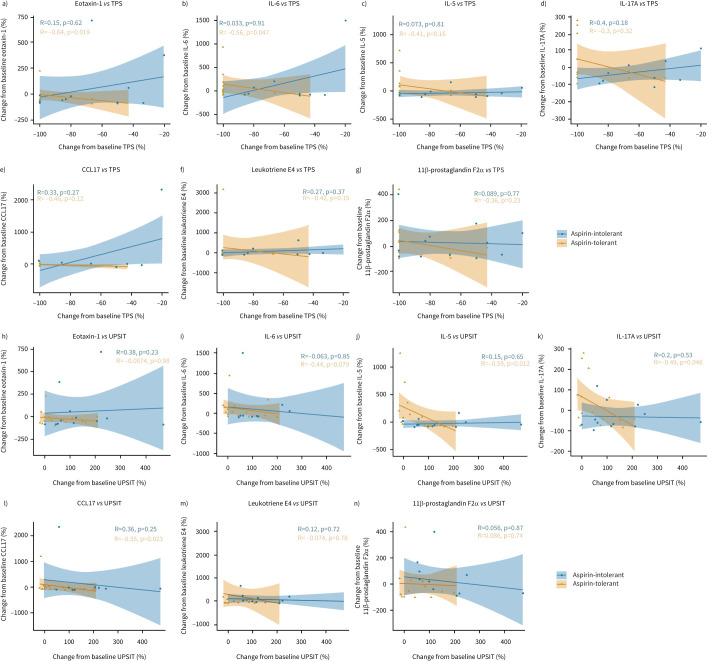
Results: Of the 31 patients included in the study, 30 completed both aspirin provocation tests. After 6 months of treatment with dupilumab, 23% of patients (n=7 of 30) developed complete aspirin tolerance and an additional 33% of patients (n=10 of 30) tolerated higher doses. Polyp burden was significantly reduced (total polyp score: -2.68±1.84, p<0.001), while pulmonary symptoms (asthma control test: +2.34±3.67, p<0.001) and olfactory performance improved (University of Pennsylvania Smell Identification Test: +11.16±9.54, p<0.001) in all patients after therapy. Patients with increased aspirin tolerance showed a significant decrease in urinary leukotriene E4 levels and their improvement in clinical parameters was associated with a reduction of eotaxin-1, C-C motif chemokine ligand 17, IL-5, IL-17A and IL-6.
Conclusion: In this study, 57% of N-ERD patients tolerated higher doses of aspirin under dupilumab therapy.
Copyright ©The authors 2023.
Conflict of interest statement
Conflict of interest: S. Schneider served as a speaker and/or consultant and/or advisory board member for Sanofi and Novartis; and is an investigator for Novartis and AstraZeneca (grants paid to his institution). T. Bartosik received personal fees from Sanofi. L.D. Landegger served as an independent consultant for Conclave Capital and Gerson Lehrman Group, is an investigator for Decibel Therapeutics and Amgen (grants paid to his institution), and acts as Chair of the Membership Committee for Association for Research in Otolaryngology (ARO). M. Rocha-Hasler reports grants from AstraZeneca. C. Bangert has received personal fees from Mylan, LEO Pharma, Pfizer, Sanofi Genzyme, Eli Lilly, Novartis, AstraZeneca and AbbVie, and is an investigator for Novartis, Sanofi, AbbVie, Elli Lilly, LEO Pharma and Galderma (grants paid to her institution). J. Eckl-Dorna served as a speaker and/or consultant and/or advisory board member for Sanofi, Allergopharma, AstraZeneca, GSK, Bencard and Novartis, and is an investigator for Novartis and AstraZeneca (grants paid to her institution). All other authors declare no conflict of interest.
Figures
Comment in
-
NSAID-exacerbated respiratory disease, dupilumab and aspirin tolerance.Eur Respir J. 2023 Mar 16;61(3):2202467. doi: 10.1183/13993003.02467-2022. Print 2023 Mar. Eur Respir J. 2023. PMID: 36927861 No abstract available.