

Plasmodium infection is associated with cross-reactive antibodies to carbohydrate epitopes on the SARS-CoV-2 Spike protein
- PMID: 36550362
- PMCID: PMC9778468
- DOI: 10.1038/s41598-022-26709-7
Plasmodium infection is associated with cross-reactive antibodies to carbohydrate epitopes on the SARS-CoV-2 Spike protein
Abstract
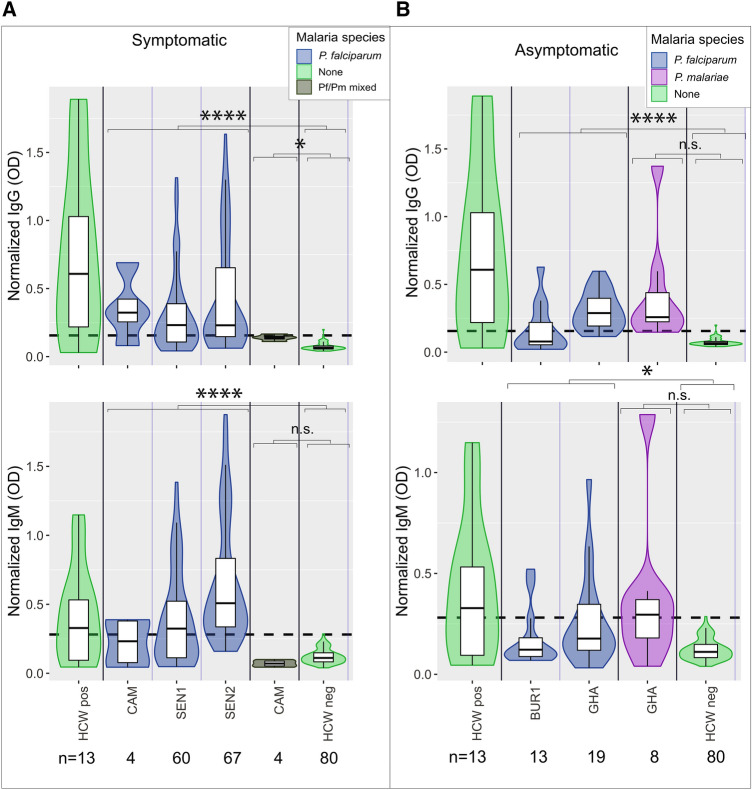
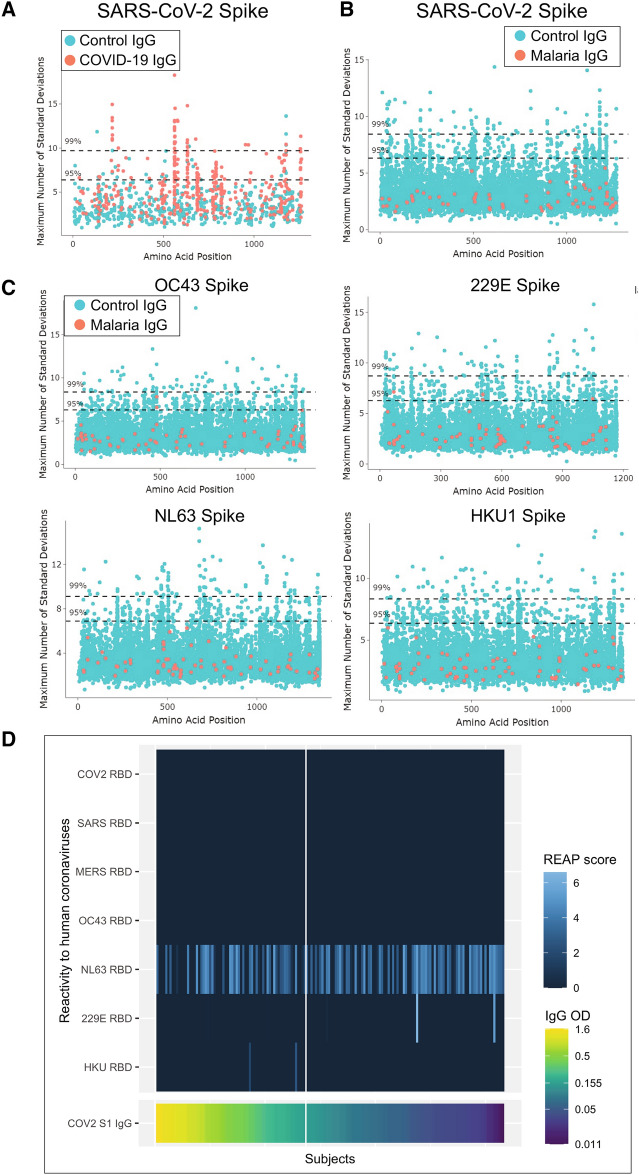
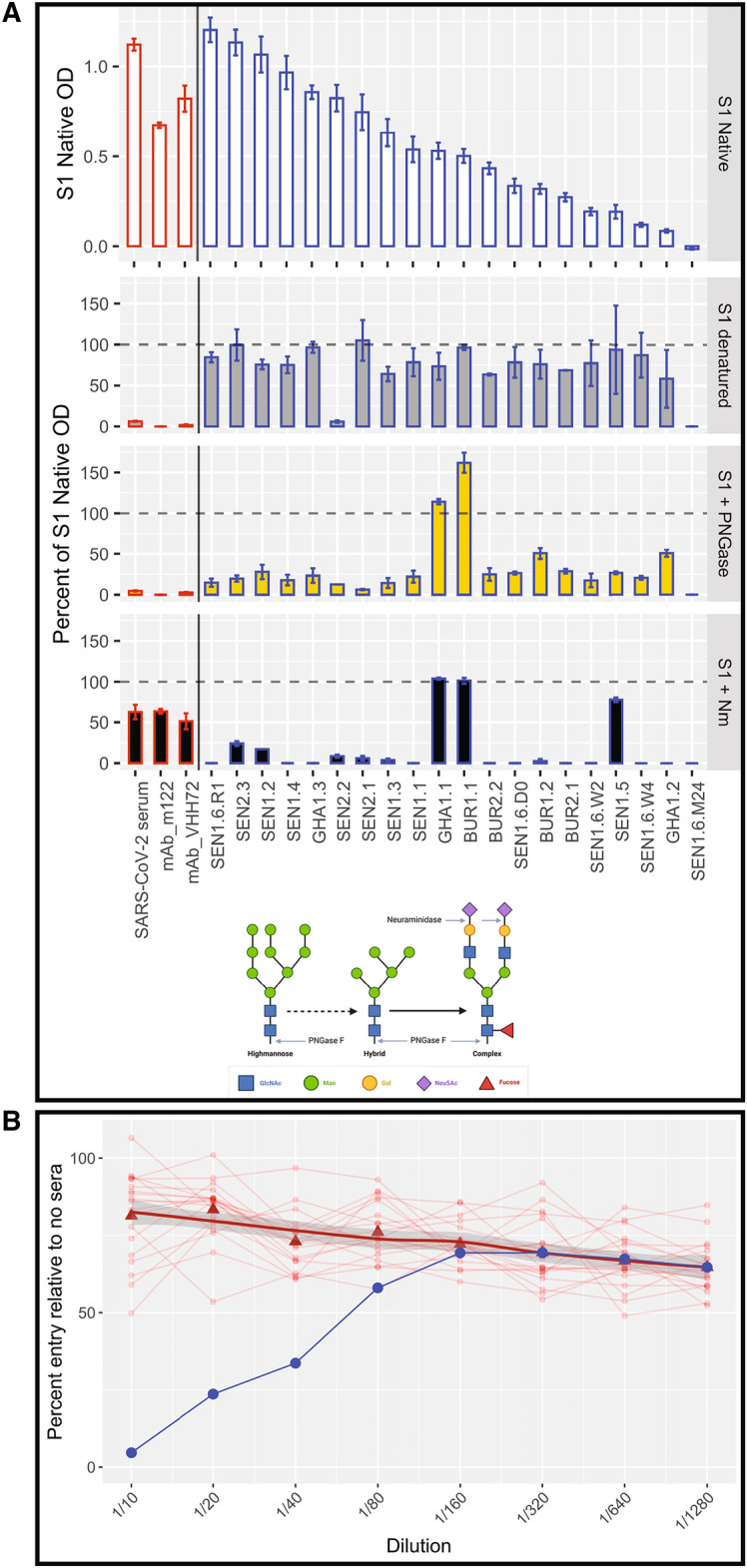
Sero-surveillance can monitor and project disease burden and risk. However, SARS-CoV-2 antibody test results can produce false positive results, limiting their efficacy as a sero-surveillance tool. False positive SARS-CoV-2 antibody results are associated with malaria exposure, and understanding this association is essential to interpret sero-surveillance results from malaria-endemic countries. Here, pre-pandemic samples from eight malaria endemic and non-endemic countries and four continents were tested by ELISA to measure SARS-CoV-2 Spike S1 subunit reactivity. Individuals with acute malaria infection generated substantial SARS-CoV-2 reactivity. Cross-reactivity was not associated with reactivity to other human coronaviruses or other SARS-CoV-2 proteins, as measured by peptide and protein arrays. ELISAs with deglycosylated and desialated Spike S1 subunits revealed that cross-reactive antibodies target sialic acid on N-linked glycans of the Spike protein. The functional activity of cross-reactive antibodies measured by neutralization assays showed that cross-reactive antibodies did not neutralize SARS-CoV-2 in vitro. Since routine use of glycosylated or sialated assays could result in false positive SARS-CoV-2 antibody results in malaria endemic regions, which could overestimate exposure and population-level immunity, we explored methods to increase specificity by reducing cross-reactivity. Overestimating population-level exposure to SARS-CoV-2 could lead to underestimates of risk of continued COVID-19 transmission in sub-Saharan Africa.
© 2022. The Author(s).
Conflict of interest statement
A.M.R. and Y.D. (Yale University) are named inventors on a patent application describing the REAP technology. A.M.R. is the founder of Seranova Bio. C.B.W. (Yale University)has a patent pending entitled “Compounds and Compositions for Treating, Ameliorating, and/or Preventing SARS-CoV-2 Infection and/or Complications Thereof". KK, EBJ, and JS receive salary and hold stock options from Serimmune Inc.
Figures



Update of
-
Plasmodium infection induces cross-reactive antibodies to carbohydrate epitopes on the SARS-CoV-2 Spike protein.medRxiv [Preprint]. 2021 May 12:2021.05.10.21256855. doi: 10.1101/2021.05.10.21256855. medRxiv. 2021. Update in: Sci Rep. 2022 Dec 22;12(1):22175. doi: 10.1038/s41598-022-26709-7. PMID: 34013301 Free PMC article. Updated. Preprint.
References
-
- Chibwana MG, et al. High SARS-CoV-2 seroprevalence in health care workers but relatively low numbers of deaths in urban Malawi. Wellcome Open Res. 2020;5:199. doi: 10.12688/wellcomeopenres.16188.2. - DOI
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
