

Flow-diverter treatment for renal artery aneurysms: One-year follow-up of a multicentric preliminary experience
- PMID: 36550762
- PMCID: PMC9885726
- DOI: 10.5152/dir.2022.211015
Flow-diverter treatment for renal artery aneurysms: One-year follow-up of a multicentric preliminary experience
Abstract
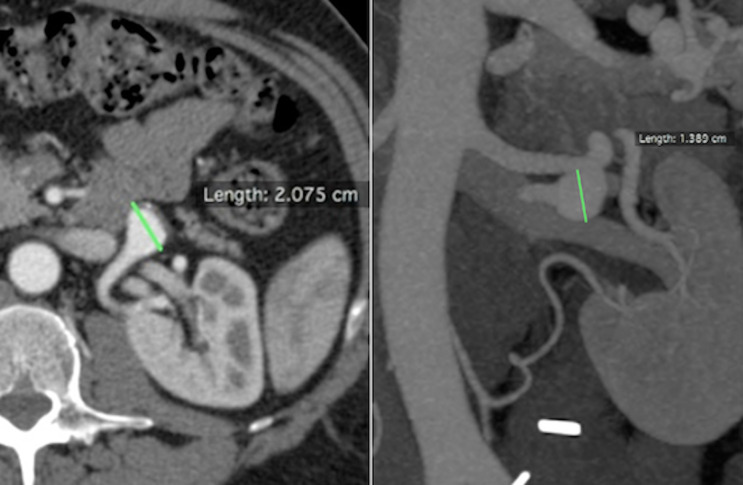
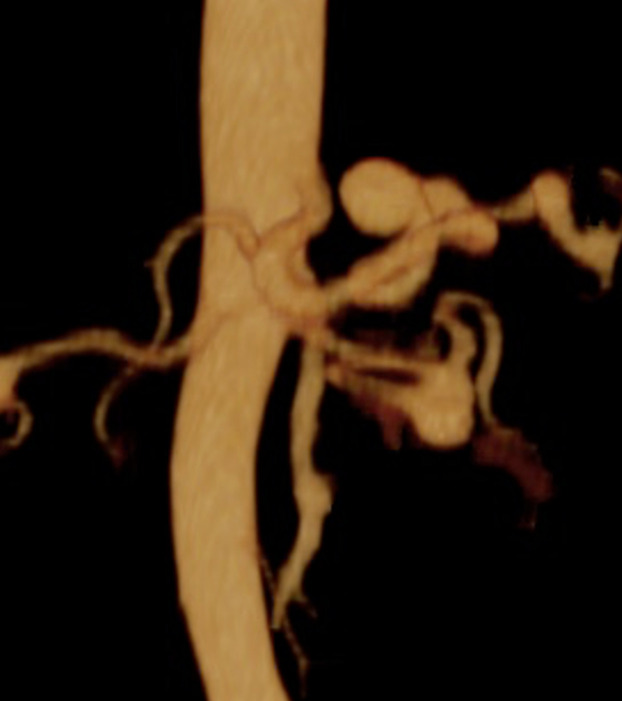
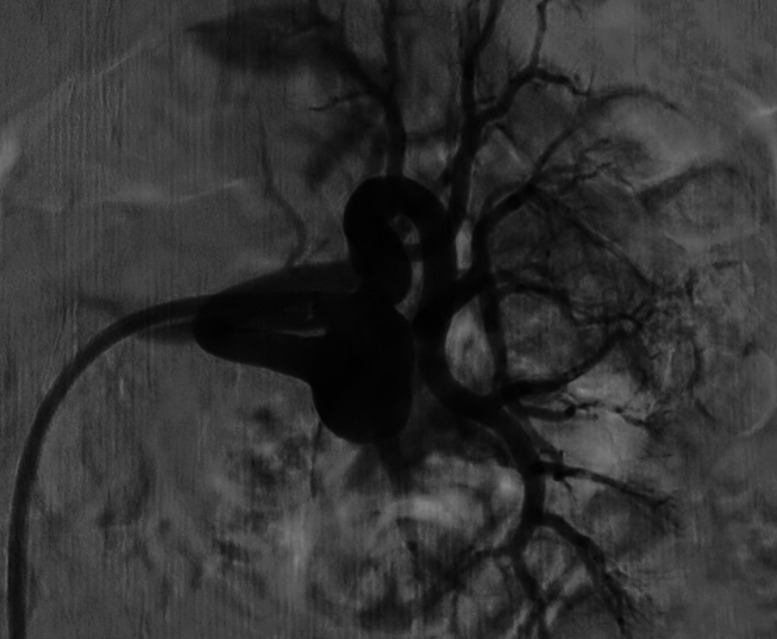
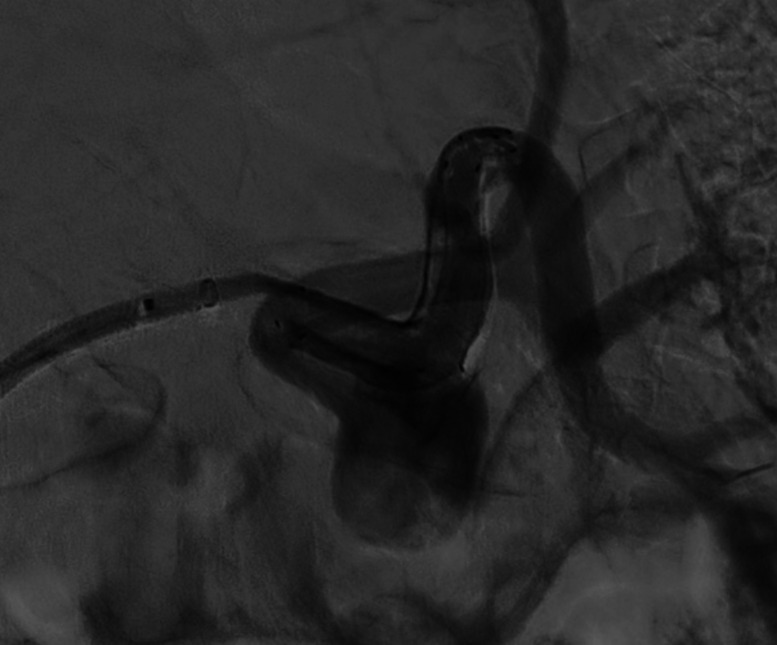
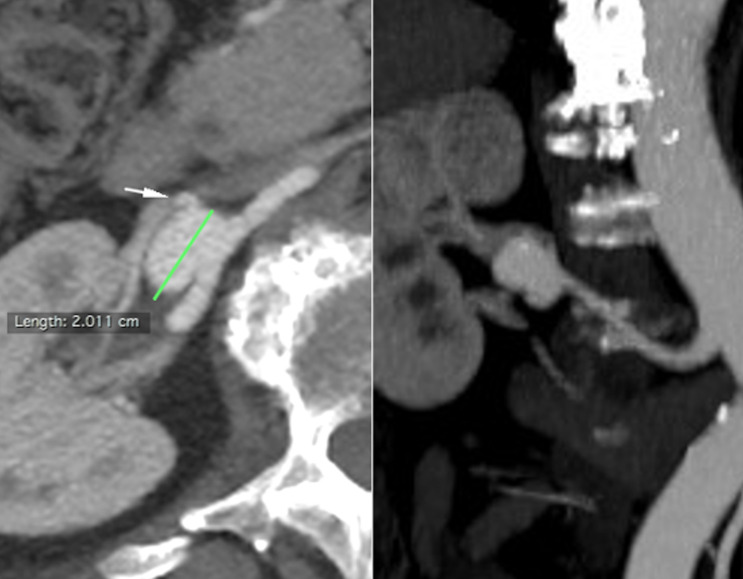
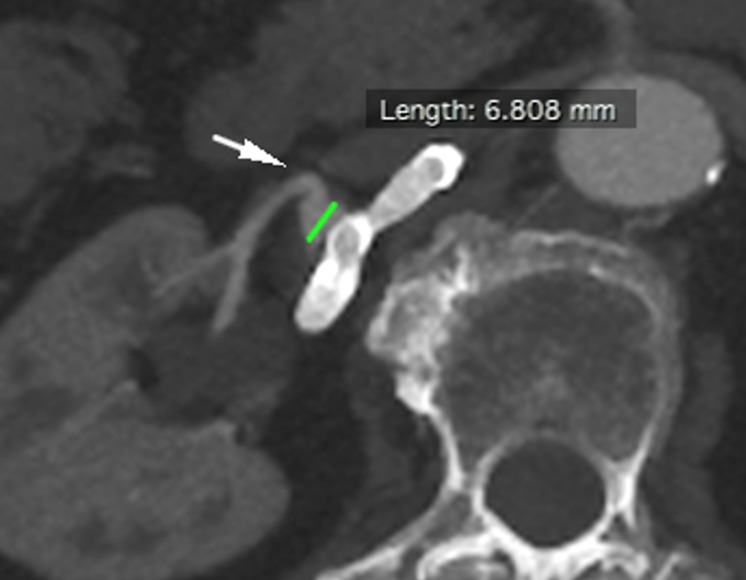
PURPOSE Renal artery aneurysms (RAAs) are rare in the general population, although the true incidence and natural history remain elusive. Conventional endovascular therapies such as coil embolization or covered stent graft may cause sidebranches occlusion, leading to organ infarction. Flow-diverters (FD) have been firstly designed to treat cerebrovascular aneurysms, but their use may be useful to treat complex RAAs presenting sidebraches arising from aneurysmal sac. To evaluate mid-term follow-up (FUP) safety and efficacy of FD during treatment of complex RAAs. METHODS Between November 2019 and April 2020, 7 RAAs were identified in 7 patients (4 men, 3 women; age range 55-82 years; median 67 years) and treated by FD. Procedural details, complications, morbidity and mortality, aneurysm occlusion and segmental artery patency were retrospectively reviewed. Twelve months computed tomography angiography (CTA) FUP was evaluated for all cases. RESULT Deployment of FD was successful in all cases. One intraprocedural technical complication was encountered with one FD felt down into aneurism sac which requiring additional telescopic stenting. One case at 3 months CTA FUP presented same complication, requiring same rescue technique. At 12 months CTA FUP 5 cases of size shrinkage and 2 cases of stable size were documented. No rescue surgery or major intraprocedural or mid-term FUP complication was seen. CONCLUSION Complex RAAs with two or more sidebranches can be safely treated by FD. FD efficacy for RAA needs a further validation at long term FUP by additional large prospective studies.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
