

Transcutaneous electrical acupoint stimulation for the prevention of perioperative neurocognitive disorders in geriatric patients: A systematic review and meta-analysis of randomized controlled trials
- PMID: 36550918
- PMCID: PMC9771360
- DOI: 10.1097/MD.0000000000032329
Transcutaneous electrical acupoint stimulation for the prevention of perioperative neurocognitive disorders in geriatric patients: A systematic review and meta-analysis of randomized controlled trials
Abstract
Background: To evaluate whether transcutaneous electrical acupoint stimulation (TEAS) decreases rates of perioperative neurocognitive disorders (PND) when used as an adjuvant method during perioperative period in geriatric patients since the new definition was released in 2018.
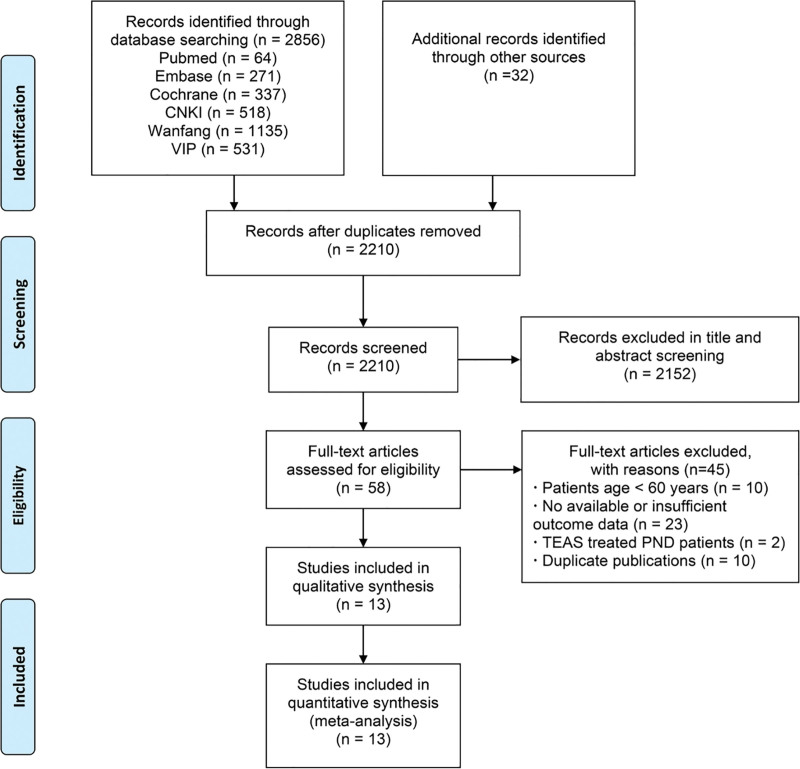
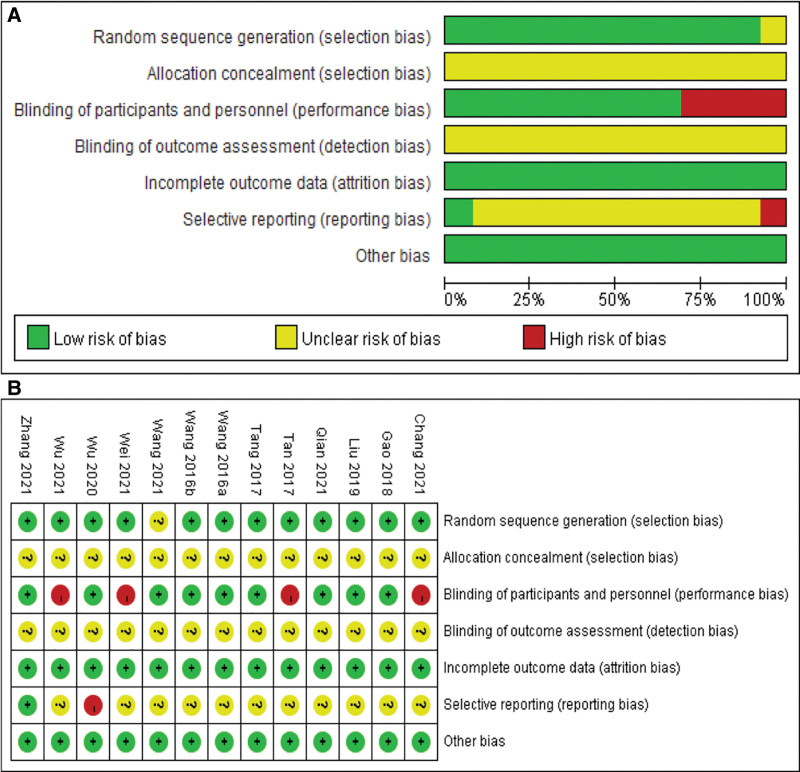
Methods: Six databases [Chinese National Knowledge Infrastructure, VIP Database for Chinese Technical Periodicals, WanFang Database, PubMed, EMBASE, and Cochrane Library] were systematically searched. Data analysis was performed using RevMan 5.4.1 software (Copenhagen: The Nordic Cochrane Centre, the Cochrane Collaboration, 2020). Risk ratios (RR) with 95% confidence interval were calculated using a random effects model. Quality of evidence was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach.
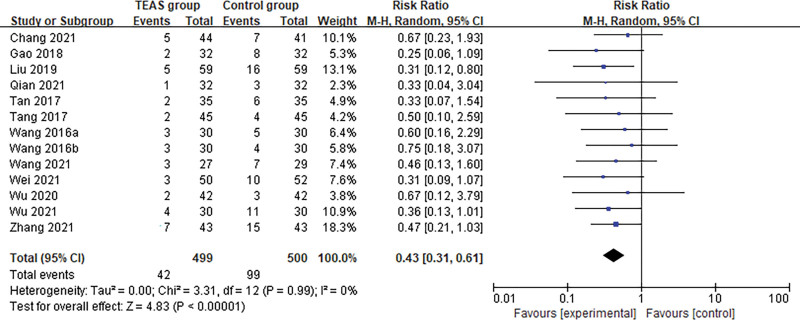
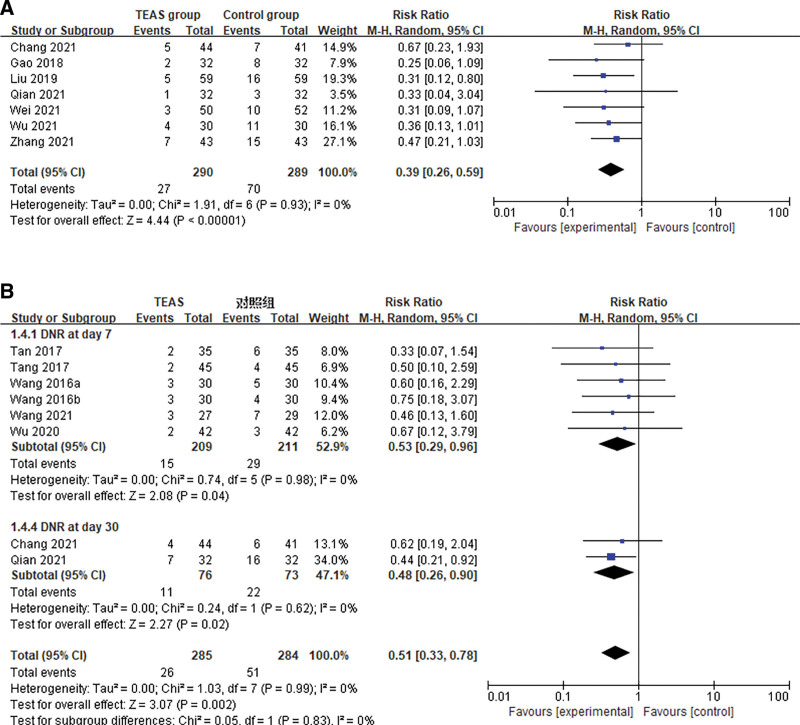
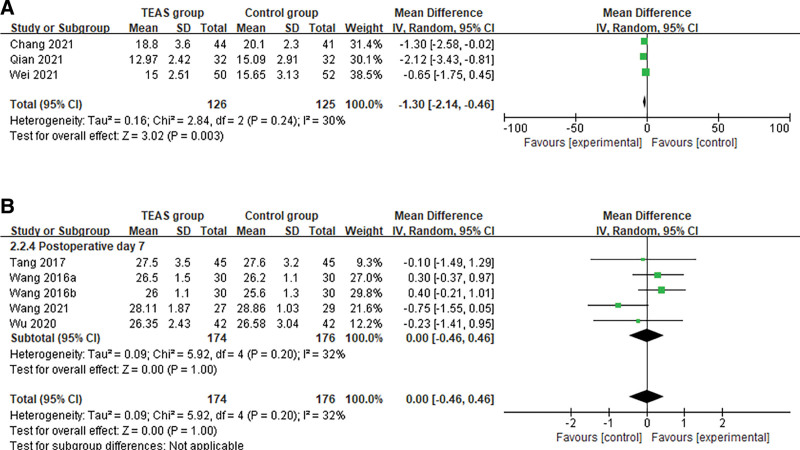
Results: 13 randomized clinical trials (999 patients) in total were included. TEAS had positive effects on preventing the incidence of PND (RR: 0.43; 0.31, 0.61; P < .001; low certainty) [postoperative delirium within 7 days (RR: 0.39; 0.26, 0.59; P < .001), delayed neurocognitive recovery within 3 months (RR: 0.51; 0.33, 0.78; P = .002)]. TEAS could also improve the scores of the confusion assessment method (CAM) (Mean difference: -1.30; -2.14, -0.46; P = .003; low certainty). Limited evidence suggested that TEAS could reduce the serum levels of biochemical indicator (S100β) (SMD = -1.08, -1.67, -0.49, P < .001; I2 = 83%; very low certainty) as well as anesthetic requirements (remifentanil) (SMD: -1.58; -2.54, -0.63; P = .001; I2 = 87%; very low certainty). Subgroup analysis indicated that different protocols of TEAS had significant pooled benefits (TEAS used only in surgery and in combination with postoperative intervention) (RR: 0.45; 0.31, 0.63; P < .001). Acupoint combination (LI4 and PC6) in the TEAS group had more significantly advantages (RR: 0.34; 0.17, 0.67; P = .002). TEAS group had a lower incidence of PND in different surgery type (orthopedic surgery and abdominal surgery) (RR: 0.43; 0.30, 0.60; P < .001), as well as with different anesthetic modality (intravenous anesthesia and intravenous and inhalational combined anesthesia) (RR: 0.38; 0.23, 0.61; P < .001).
Conclusion: In terms of clinical effectiveness, TEAS appeared to be beneficial for prophylaxis of PND during a relatively recent period, noting the limitations of the current evidence.
Copyright © 2022 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Authors declare that there are no conflicts of interest regarding the publication of this paper. Statement of human and animal rights: This article does not contain any studies with human participants or animals performed by any of the authors.
Figures
Similar articles
-
Electroacupuncture and Transcutaneous Electrical Acupoint Stimulation for Perioperative Neurocognitive Disorder in Older Patients Undergoing Cardiac Surgery: Protocol for Systematic Review and Meta-Analysis.JMIR Res Protoc. 2024 Aug 29;13:e55996. doi: 10.2196/55996. JMIR Res Protoc. 2024. PMID: 39208417 Free PMC article.
-
Intraoperative transcutaneous electrical acupoint stimulation combined with anesthesia to prevent postoperative cognitive dysfunction: A systematic review and meta-analysis.PLoS One. 2025 Jan 9;20(1):e0313622. doi: 10.1371/journal.pone.0313622. eCollection 2025. PLoS One. 2025. PMID: 39787088 Free PMC article.
-
Effect of Transcutaneous Electrical Acupoint Stimulation on Extubation-Related Stress Response in Noncardiac Surgery Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials.J Perianesth Nurs. 2024 Dec;39(6):990-998. doi: 10.1016/j.jopan.2024.01.015. Epub 2024 Jun 19. J Perianesth Nurs. 2024. PMID: 38904602
-
Effect of transcutaneous electrical acupoint stimulation on postoperative pain in pediatric orthopedic surgery with the enhanced recovery after surgery protocol: a prospective, randomized controlled trial.Anaesth Crit Care Pain Med. 2023 Dec;42(6):101273. doi: 10.1016/j.accpm.2023.101273. Epub 2023 Jul 5. Anaesth Crit Care Pain Med. 2023. PMID: 37419321
-
Evaluation of transcutaneous electrical acupoint stimulation for improving pain and cognitive function in elderly patients around the perioperative period of hip replacement surgery: A meta-analysis.PLoS One. 2024 Oct 21;19(10):e0309673. doi: 10.1371/journal.pone.0309673. eCollection 2024. PLoS One. 2024. PMID: 39432497 Free PMC article.
Cited by
-
The research progress of perioperative non-pharmacological interventions on postoperative cognitive dysfunction: a narrative review.Front Neurol. 2024 May 1;15:1369821. doi: 10.3389/fneur.2024.1369821. eCollection 2024. Front Neurol. 2024. PMID: 38751891 Free PMC article.
-
Electroacupuncture and Transcutaneous Electrical Acupoint Stimulation for Perioperative Neurocognitive Disorder in Older Patients Undergoing Cardiac Surgery: Protocol for Systematic Review and Meta-Analysis.JMIR Res Protoc. 2024 Aug 29;13:e55996. doi: 10.2196/55996. JMIR Res Protoc. 2024. PMID: 39208417 Free PMC article.
-
Effect of Different Frequencies of Transcutaneous Electrical Acupoint Stimulation (TEAS) on EEG Source Localization in Healthy Volunteers: A Semi-Randomized, Placebo-Controlled, Crossover Study.Brain Sci. 2025 Mar 3;15(3):270. doi: 10.3390/brainsci15030270. Brain Sci. 2025. PMID: 40149791 Free PMC article.
-
Postoperative Multimodal Analgesia Strategy for Enhanced Recovery After Surgery in Elderly Colorectal Cancer Patients.Pain Ther. 2024 Aug;13(4):745-766. doi: 10.1007/s40122-024-00619-0. Epub 2024 Jun 5. Pain Ther. 2024. PMID: 38836984 Free PMC article. Review.
-
Intraoperative transcutaneous electrical acupoint stimulation combined with anesthesia to prevent postoperative cognitive dysfunction: A systematic review and meta-analysis.PLoS One. 2025 Jan 9;20(1):e0313622. doi: 10.1371/journal.pone.0313622. eCollection 2025. PLoS One. 2025. PMID: 39787088 Free PMC article.
References
-
- Gustafson Y, Berggren D, Brännström B, et al. . Acute confusional states in elderly patients treated for femoral neck fracture. J Am Geriatr Soc. 1988;36:525–30. - PubMed
-
- O’Keeffe ST, Ní CA. Postoperative delirium in the elderly. Br J Anaesth. 1994;73:673–87. - PubMed
-
- Moller JT, Cluitmans P, Rasmussen LS, et al. . Long-term postoperative cognitive dysfunction in the elderly ISPOCD1 study. ISPOCD investigators. International study of post-operative cognitive dysfunction. Lancet. 1998;351:857–61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
