

Genetic Ablation of Ankrd1 Mitigates Cardiac Damage during Experimental Autoimmune Myocarditis in Mice
- PMID: 36551326
- PMCID: PMC9775225
- DOI: 10.3390/biom12121898
Genetic Ablation of Ankrd1 Mitigates Cardiac Damage during Experimental Autoimmune Myocarditis in Mice
Abstract
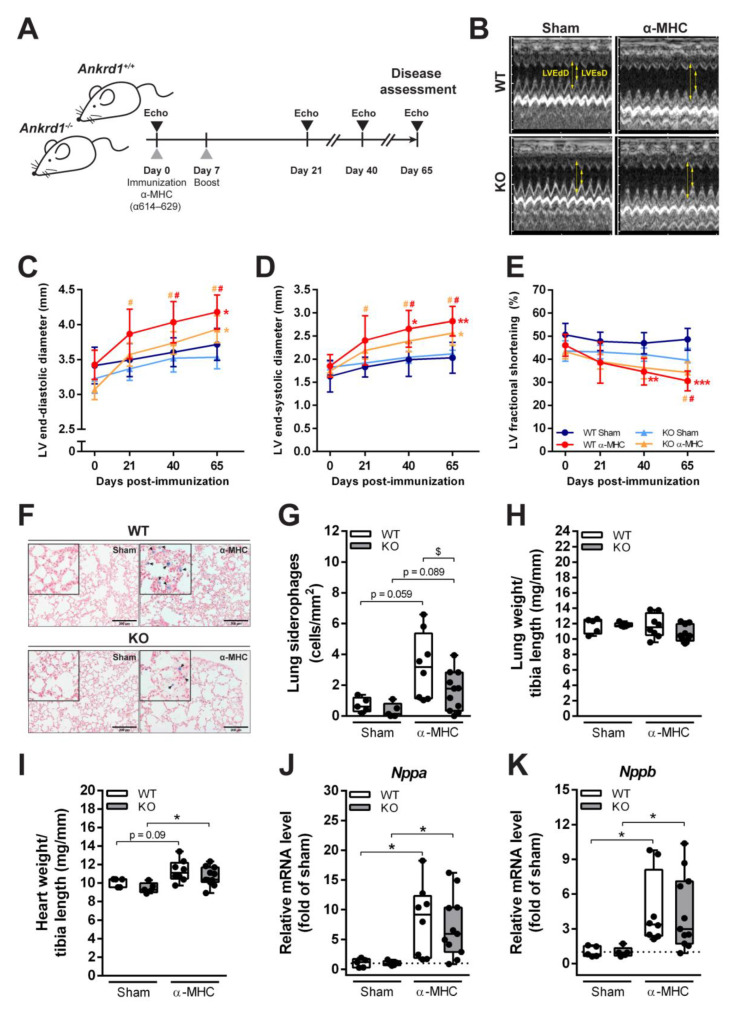
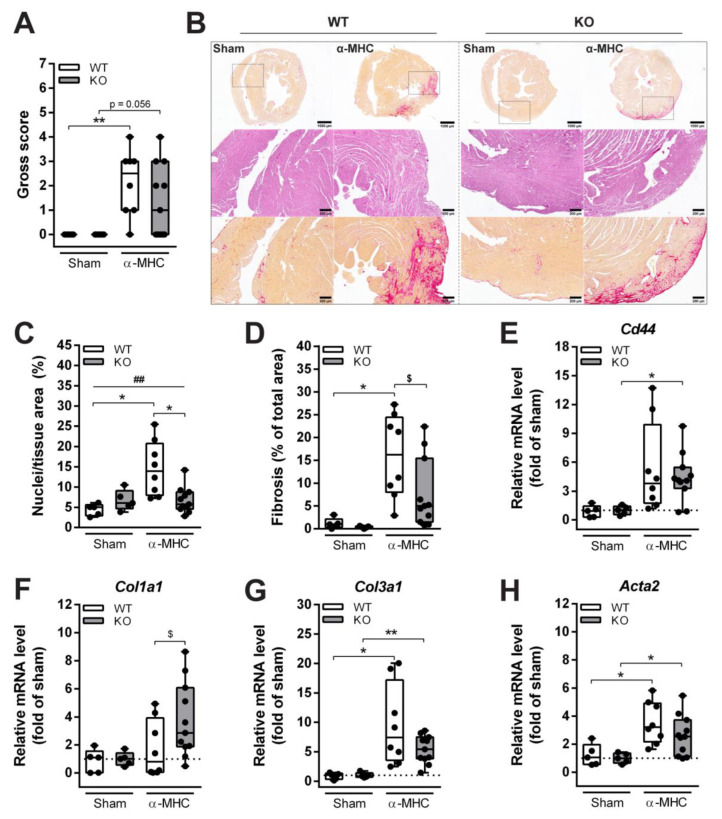
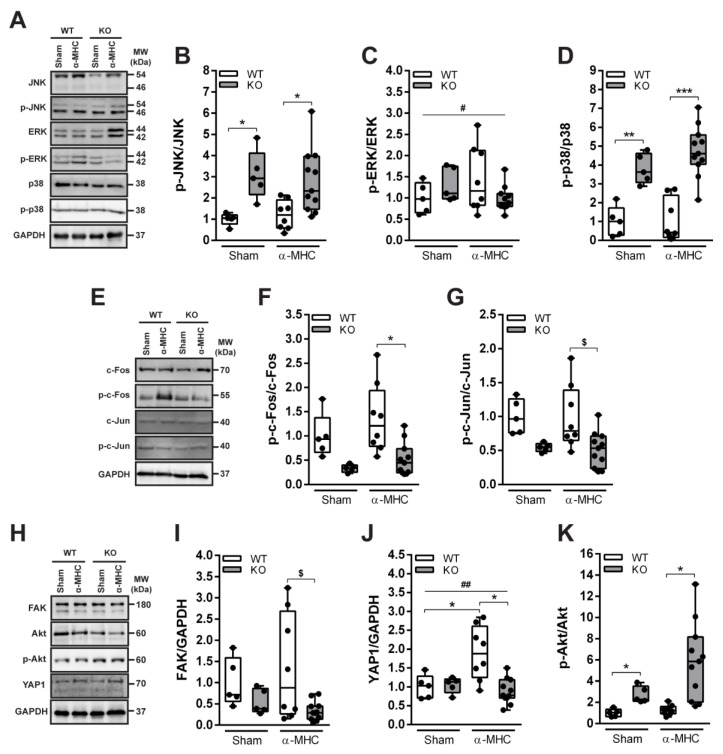
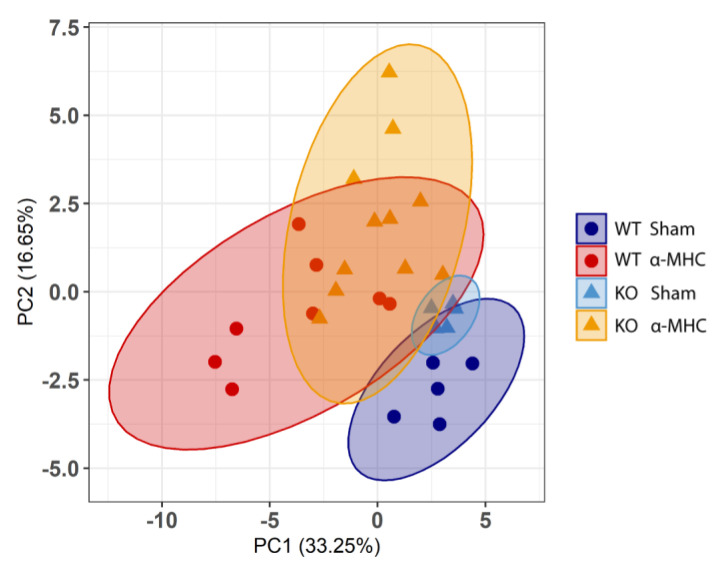
Myocarditis (MC) is an inflammatory disease of the myocardium that can cause sudden death in the acute phase, and dilated cardiomyopathy (DCM) with chronic heart failure as its major long-term outcome. However, the molecular mechanisms beyond the acute MC phase remain poorly understood. The ankyrin repeat domain 1 (ANKRD1) is a functionally pleiotropic stress/stretch-inducible protein, which can modulate cardiac stress response during various forms of pathological stimuli; however, its involvement in post-MC cardiac remodeling leading to DCM is not known. To address this, we induced experimental autoimmune myocarditis (EAM) in ANKRD1-deficient mice, and evaluated post-MC consequences at the DCM stage mice hearts. We demonstrated that ANKRD1 does not significantly modulate heart failure; nevertheless, the genetic ablation of Ankrd1 blunted the cardiac damage/remodeling and preserved heart function during post-MC DCM.
Keywords: ANKRD1; dilated cardiomyopathy; heart failure; inflammation; myocardial remodeling; myocarditis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Inflammatory dilated cardiomyopathy (DCMI).Herz. 2005 Sep;30(6):535-44. doi: 10.1007/s00059-005-2730-5. Herz. 2005. PMID: 16170686 Review.
-
[Familial predisposition and microbial etiology in dilated cardiomyopathy].Herz. 2009 Mar;34(2):110-6. doi: 10.1007/s00059-009-3200-2. Herz. 2009. PMID: 19370326 German.
-
Myocardial-specific ablation of Jumonji and AT-rich interaction domain-containing 2 (Jarid2) leads to dilated cardiomyopathy in mice.J Biol Chem. 2019 Mar 29;294(13):4981-4996. doi: 10.1074/jbc.RA118.005634. Epub 2019 Jan 30. J Biol Chem. 2019. PMID: 30700554 Free PMC article.
-
ANKRD1, the gene encoding cardiac ankyrin repeat protein, is a novel dilated cardiomyopathy gene.J Am Coll Cardiol. 2009 Jul 21;54(4):325-33. doi: 10.1016/j.jacc.2009.02.076. J Am Coll Cardiol. 2009. PMID: 19608030 Free PMC article.
-
Regulation of inflammation and myocardial fibrosis in experimental autoimmune myocarditis.Inflamm Allergy Drug Targets. 2011 Jun;10(3):218-25. doi: 10.2174/187152811795564091. Inflamm Allergy Drug Targets. 2011. PMID: 21495969 Review.
Cited by
-
Mechanisms underlying dilated cardiomyopathy associated with FKBP12 deficiency.J Gen Physiol. 2025 Jan 6;157(1):e202413583. doi: 10.1085/jgp.202413583. Epub 2024 Dec 11. J Gen Physiol. 2025. PMID: 39661086 Free PMC article.
-
Research progress of ankyrin repeat domain 1 protein: an updated review.Cell Mol Biol Lett. 2024 Oct 17;29(1):131. doi: 10.1186/s11658-024-00647-w. Cell Mol Biol Lett. 2024. PMID: 39420247 Free PMC article. Review.
References
-
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study. Lancet. 2018;392:1789–1858. doi: 10.1016/S0140-6736(18)32279-7. - DOI - PMC - PubMed
-
- Ammirati E., Frigerio M., Adler E.D., Basso C., Birnie D.H., Brambatti M., Friedrich M.G., Klingel K., Lehtonen J., Moslehi J.J., et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy. Circ. Heart Fail. 2020;13:e007405. doi: 10.1161/CIRCHEARTFAILURE.120.007405. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
