

Epidemiology of Merkel Cell Polyomavirus Infection and Merkel Cell Carcinoma
- PMID: 36551657
- PMCID: PMC9776808
- DOI: 10.3390/cancers14246176
Epidemiology of Merkel Cell Polyomavirus Infection and Merkel Cell Carcinoma
Abstract
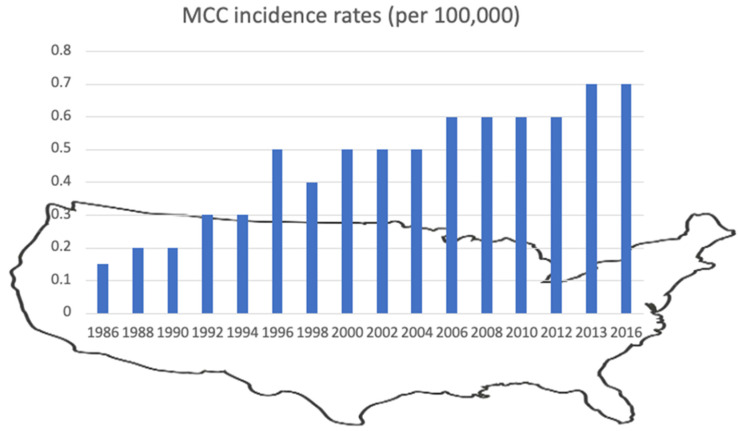
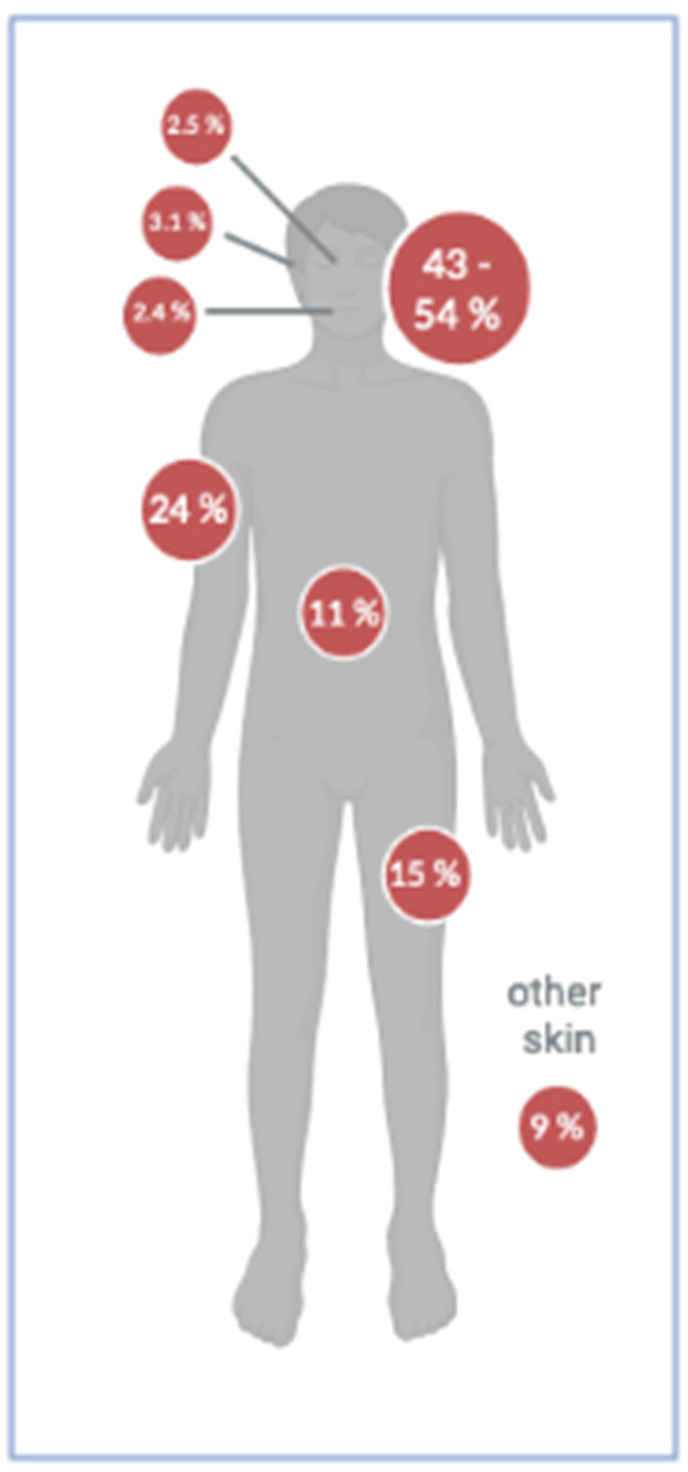
Merkel cell polyomavirus (MCPyV) is a ubiquitous virus replicating in human dermal fibroblasts. MCPyV DNA can be detected on healthy skin in 67−90% of various body sites, and intact virions are regularly shed from the skin. Infection occurs early in life, and seropositivity increases from 37 to 42% in 1- to 6-year-olds to 92% in adults. Merkel cell carcinoma (MCC) is a rare but very aggressive neuroendocrine tumor of the skin. It develops mainly on sun-exposed areas as a fast-growing, reddish nodule. Two MCC entities exist: about 80% of MCC are MCPyV-associated. Tumorigenesis is driven by viral integration into the host genome and MCPyV oncogene expression. In MCPyV-negative MCC, UV radiation causes extensive DNA damage leading to the deregulation of the cell cycle. In recent decades, MCC incidence rates have increased worldwide, e.g., in the United States, from 0.15 in 1986 to 0.7/100,000 in 2016. Risk factors for the development of MCC include male sex, older age (>75 years), fair skin, intense UV exposure, and immunosuppression. Projections suggest that due to aging populations, an increase in immunosuppressed patients, and enhanced UV exposure, MCC incidence rates will continue to rise. Early diagnosis and prompt treatment are crucial to reducing high MCC morbidity and mortality.
Keywords: MCC; MCPyV; Merkel cell carcinoma; Merkel cell polyomavirus; epidemiology.
Conflict of interest statement
The authors declare no conflict of interest.
Figures



Similar articles
-
Merkel Cell Polyomavirus Infection Induces an Antiviral Innate Immune Response in Human Dermal Fibroblasts.J Virol. 2021 Jun 10;95(13):e0221120. doi: 10.1128/JVI.02211-20. Epub 2021 Jun 10. J Virol. 2021. PMID: 33883226 Free PMC article.
-
Characterization of the Impact of Merkel Cell Polyomavirus-Induced Interferon Signaling on Viral Infection.J Virol. 2023 Apr 27;97(4):e0190722. doi: 10.1128/jvi.01907-22. Epub 2023 Mar 22. J Virol. 2023. PMID: 36946735 Free PMC article.
-
Merkel Cell Polyomavirus Infection of Animal Dermal Fibroblasts.J Virol. 2018 Jan 30;92(4):e01610-17. doi: 10.1128/JVI.01610-17. Print 2018 Feb 15. J Virol. 2018. PMID: 29167345 Free PMC article.
-
Merkel cell carcinoma: The first human cancer shown to be associated with a polyomavirus.Presse Med. 2014 Dec;43(12 Pt 2):e405-11. doi: 10.1016/j.lpm.2014.09.008. Epub 2014 Nov 6. Presse Med. 2014. PMID: 25455636 Review.
-
From Merkel Cell Polyomavirus Infection to Merkel Cell Carcinoma Oncogenesis.Front Microbiol. 2021 Sep 8;12:739695. doi: 10.3389/fmicb.2021.739695. eCollection 2021. Front Microbiol. 2021. PMID: 34566942 Free PMC article. Review.
Cited by
-
Serum antibodies against mimotopes of Merkel cell polyomavirus oncoproteins detected by a novel immunoassay in healthy individuals and Merkel cell carcinoma patients.Microb Biotechnol. 2024 Oct;17(10):e14536. doi: 10.1111/1751-7915.14536. Microb Biotechnol. 2024. PMID: 39460382 Free PMC article.
-
Lymphotropic polyomavirus and Merkel cell polyomavirus in patients infected with HIV or hepatitis B or C virus.New Microbes New Infect. 2024 Aug 30;62:101471. doi: 10.1016/j.nmni.2024.101471. eCollection 2024 Dec. New Microbes New Infect. 2024. PMID: 39290794 Free PMC article.
-
Merkel-cell carcinoma: ESMO-EURACAN Clinical Practice Guideline for diagnosis, treatment and follow-up.ESMO Open. 2024 May;9(5):102977. doi: 10.1016/j.esmoop.2024.102977. Epub 2024 Apr 30. ESMO Open. 2024. PMID: 38796285 Free PMC article.
-
The Role of Oncogenic Viruses in the Pathogenesis of Sporadic Breast Cancer: A Comprehensive Review of the Current Literature.Pathogens. 2024 May 25;13(6):451. doi: 10.3390/pathogens13060451. Pathogens. 2024. PMID: 38921749 Free PMC article. Review.
-
Inpatient prevalence and factors associated with Merkel Cell Carcinoma inpatient hospitalization in the United States.Arch Dermatol Res. 2024 Jul 27;316(8):489. doi: 10.1007/s00403-024-03222-7. Arch Dermatol Res. 2024. PMID: 39066821
References
-
- Yang R., Lee E.E., Kim J., Choi J.H., Kolitz E., Chen Y., Crewe C., Salisbury N.J.H., Scherer P.E., Cockerell C., et al. Characterization of ALTO-encoding circular RNAs expressed by Merkel cell polyomavirus and trichodysplasia spinulosa polyomavirus. PLoS Pathog. 2021;17:e1009582. doi: 10.1371/journal.ppat.1009582. - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
