

Pathogenesis and Current Treatment Strategies of Hepatocellular Carcinoma
- PMID: 36551958
- PMCID: PMC9775527
- DOI: 10.3390/biomedicines10123202
Pathogenesis and Current Treatment Strategies of Hepatocellular Carcinoma
Abstract
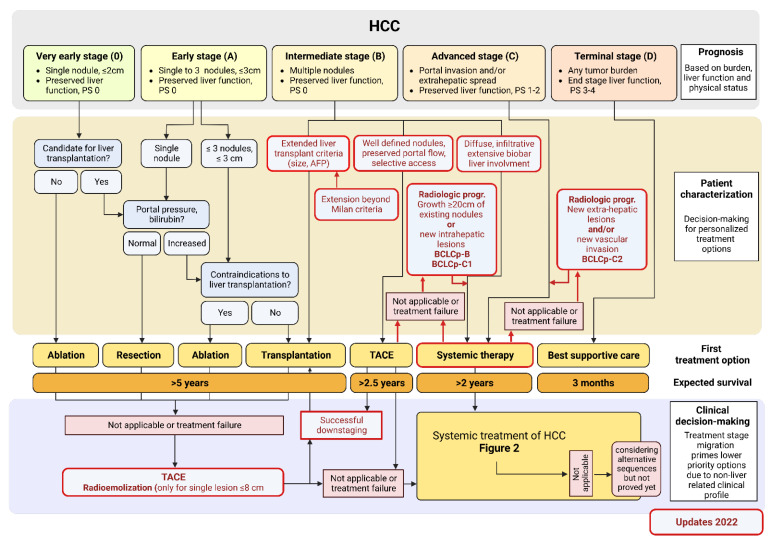
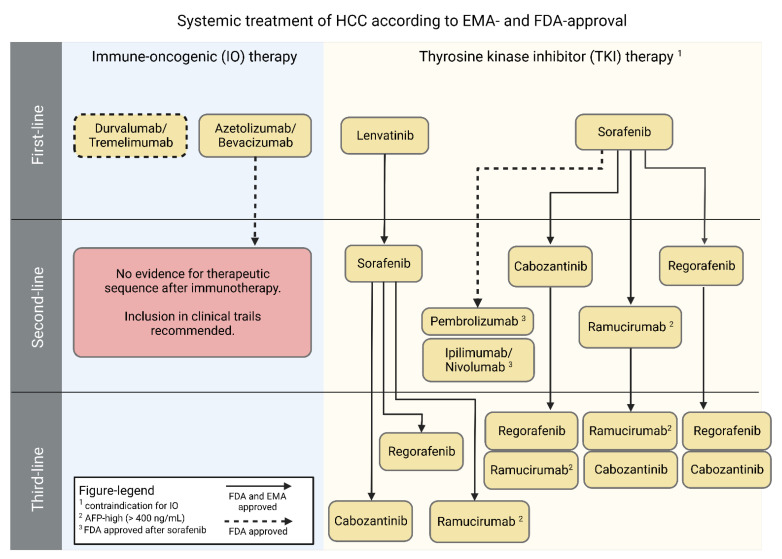
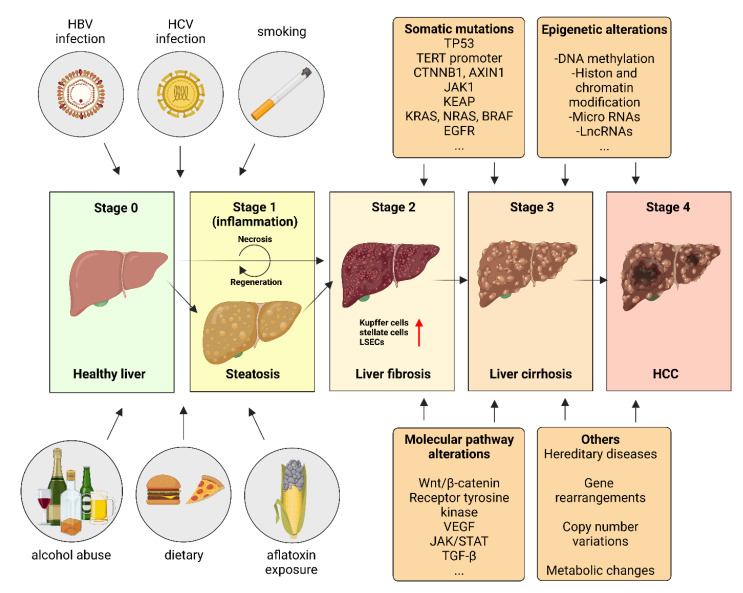
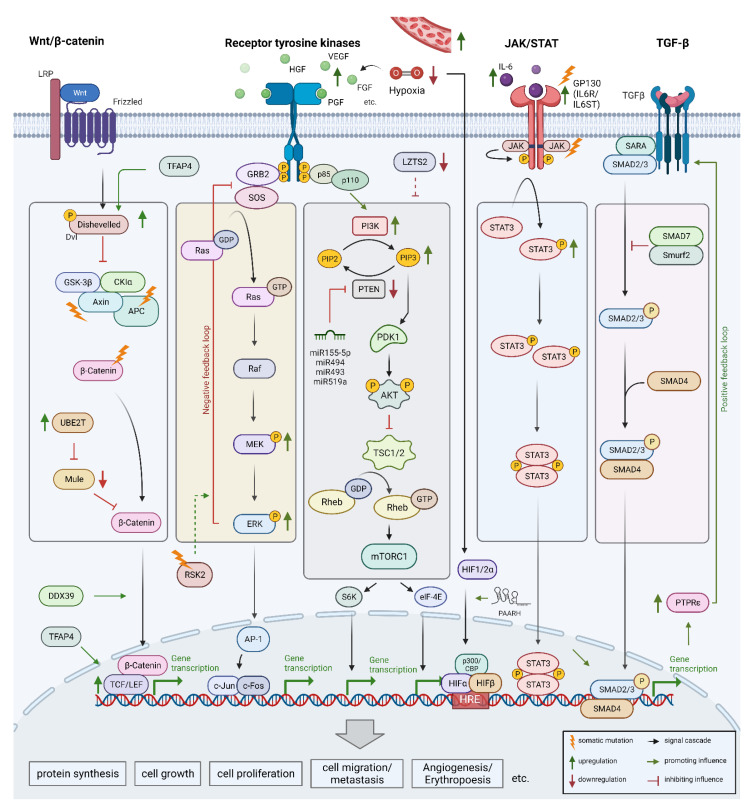
Hepatocellular carcinoma (HCC) is the most frequent liver cancer with high lethality and low five-year survival rates leading to a substantial worldwide burden for healthcare systems. HCC initiation and progression are favored by different etiological risk factors including hepatitis B virus (HBV) and hepatitis C virus (HCV) infection, non-/and alcoholic fatty liver disease (N/AFLD), and tobacco smoking. In molecular pathogenesis, endogenous alteration in genetics (TP53, TERT, CTNNB1, etc.), epigenetics (DNA-methylation, miRNA, lncRNA, etc.), and dysregulation of key signaling pathways (Wnt/β-catenin, JAK/STAT, etc.) strongly contribute to the development of HCC. The multitude and complexity of different pathomechanisms also reflect the difficulties in tailored medical therapy of HCC. Treatment options for HCC are strictly dependent on tumor staging and liver function, which are structured by the updated Barcelona Clinic Liver Cancer classification system. Surgical resection, local ablative techniques, and liver transplantation are valid and curative therapeutic options for early tumor stages. For multifocal and metastatic diseases, systemic therapy is recommended. While Sorafenib had been the standalone HCC first-line therapy for decades, recent developments had led to the approval of new treatment options as first-line as well as second-line treatment. Anti-PD-L1 directed combination therapies either with anti-VEGF directed agents or with anti-CTLA-4 active substances have been implemented as the new treatment standard in the first-line setting. However, data from clinical trials indicate different responses on specific therapeutic regimens depending on the underlying pathogenesis of hepatocellular cancer. Therefore, histopathological examinations have been re-emphasized by current international clinical guidelines in addition to the standardized radiological diagnosis using contrast-enhanced cross-sectional imaging. In this review, we emphasize the current knowledge on molecular pathogenesis of hepatocellular carcinoma. On this occasion, the treatment sequences for early and advanced tumor stages according to the recently updated Barcelona Clinic Liver Cancer classification system and the current algorithm of systemic therapy (first-, second-, and third-line treatment) are summarized. Furthermore, we discuss novel precautional and pre-therapeutic approaches including therapeutic vaccination, adoptive cell transfer, locoregional therapy enhancement, and non-coding RNA-based therapy as promising treatment options. These novel treatments may prolong overall survival rates in regard with quality of life and liver function as mainstay of HCC therapy.
Keywords: Barcelona Clinic Liver Cancer classification system (BCLC); CTLA4; HCC; NAFLD; NASH; P53; PDL1; TERT; Tyrosine kinase inhibition (TKI); atezolizumab; immune checkpoint inhibition; lenvatinib; non-alcoholic fatty liver disease; non-alcoholic steatohepatitis; pembrolizumab; trans-arterial chemoembolization (TACE).
Conflict of interest statement
A.K.: Roche Pharma AG; Eisai GmbH; Abbvie Deutschland, Janssen-Cilag; MSD Sharp & Dome, Boston Scientific Corp. Micro-Tech Europe, Fujifilm Europe, Bayer Vital GmbH (Lectures and medical advice), All other authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
