

Cranial Ultrasound Abnormalities in Small for Gestational Age or Growth-Restricted Infants Born over 32 Weeks Gestation: A Systematic Review and Meta-Analysis
- PMID: 36552172
- PMCID: PMC9776358
- DOI: 10.3390/brainsci12121713
Cranial Ultrasound Abnormalities in Small for Gestational Age or Growth-Restricted Infants Born over 32 Weeks Gestation: A Systematic Review and Meta-Analysis
Abstract
Aim: To perform a systematic review and meta-analysis of existing literature to evaluate the incidence of cranial ultrasound abnormalities (CUAs) amongst moderate to late preterm (MLPT) and term infants, affected by fetal growth restriction (FGR) or those classified as small for gestational age (SGA).
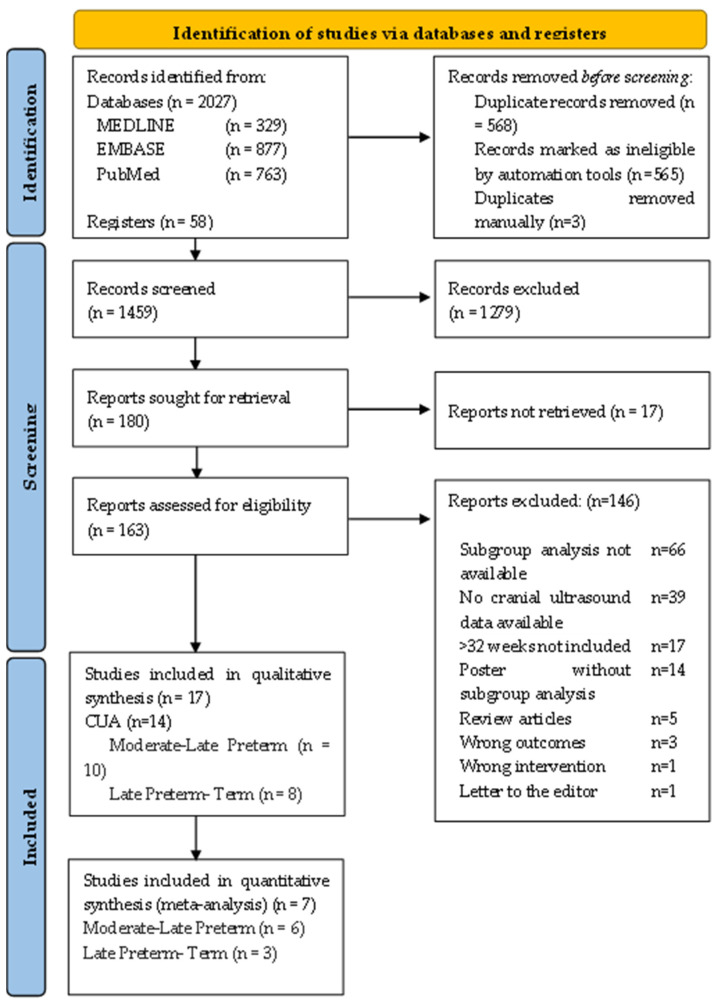
Methods: A systematic review methodology was performed, and Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement was utilised. Descriptive and observational studies reporting cranial ultrasound outcomes on FGR/SGA MLPT and term infants were included. Primary outcomes reported was incidence of CUAs in MLPT and term infants affected by FGR or SGA, with secondary outcomes including brain structure development and growth, and cerebral artery Dopplers. A random-effects model meta-analysis was performed. Risk of Bias was assessed using the Newcastle-Ottawa scale for case-control and cohort studies, and Joanna Briggs Institute Critical Appraisal Checklist for studies reporting prevalence data. GRADE was used to assess for certainty of evidence.
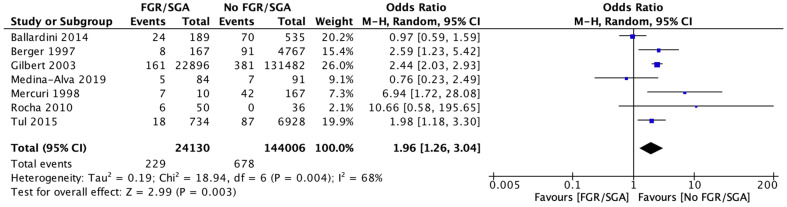
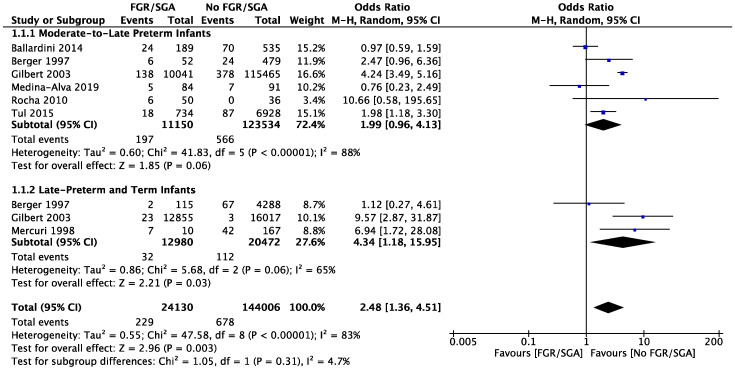
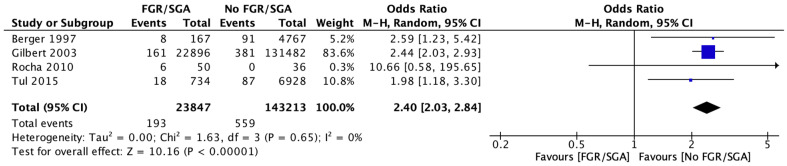
Results: Out of a total of 2085 studies identified through the search, seventeen were deemed to be relevant and included. Nine studies assessed CUAs in MLPT FGR/SGA infants, seven studies assessed CUAs in late preterm and term FGR/SGA infants, and one study assessed CUAs in both MLPT and term FGR/SGA infants. The incidence of CUAs in MLPT, and late preterm to term FGR/SGA infants ranged from 0.4 to 33% and 0 to 70%, respectively. A meta-analysis of 7 studies involving 168,136 infants showed an increased risk of any CUA in FGR infants compared to appropriate for gestational age (AGA) infants (RR 1.96, [95% CI 1.26-3.04], I2 = 68%). The certainty of evidence was very low due to non-randomised studies, methodological limitations, and heterogeneity. Another meta-analysis looking at 4 studies with 167,060 infants showed an increased risk of intraventricular haemorrhage in FGR/SGA infants compared to AGA infants (RR 2.40, [95% CI 2.03-2.84], I2 = 0%). This was also of low certainty.
Conclusions: The incidence of CUAs in MLPT and term growth-restricted infants varied widely between studies. Findings from the meta-analyses suggest the risk of CUAs and IVH may indeed be increased in these FGR/SGA infants when compared with infants not affected by FGR, however the evidence is of low to very low certainty. Further specific cohort studies are needed to fully evaluate the benefits and prognostic value of cranial ultrasonography to ascertain the need for, and timing of a cranial ultrasound screening protocol in this infant population, along with follow-up studies to ascertain the significance of CUAs identified.
Keywords: fetal growth restriction; intrauterine growth restriction; intraventricular haemorrhage; moderate-late preterm; neonate; periventricular leukomalacia; term.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
