

Endoscopic Diagnosis of Eosinophilic Esophagitis: Basics and Recent Advances
- PMID: 36553209
- PMCID: PMC9777529
- DOI: 10.3390/diagnostics12123202
Endoscopic Diagnosis of Eosinophilic Esophagitis: Basics and Recent Advances
Abstract
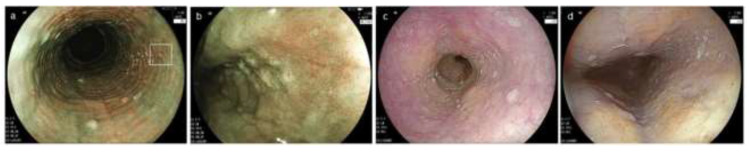
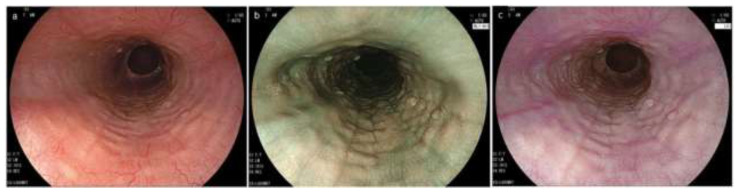
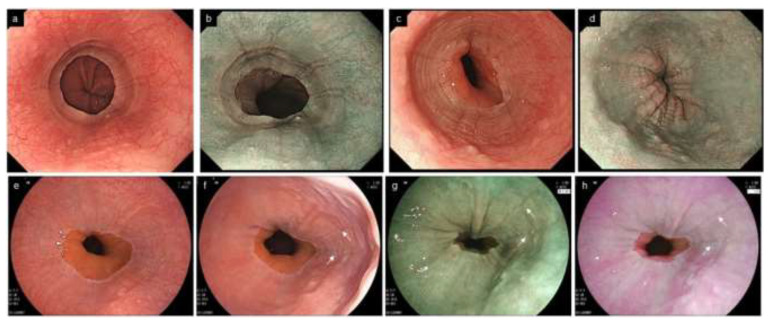
Eosinophilic esophagitis (EoE) is a chronic, immune-mediated inflammatory disease, characterized by esophageal dysfunction and intense eosinophil infiltration localized in the esophagus. In recent decades, EoE has become a growing concern as a major cause of dysphagia and food impaction in adolescents and adults. EoE is a clinicopathological disease for which the histological demonstration of esophageal eosinophilia is essential for diagnosis. Therefore, the recognition of the characteristic endoscopic features with subsequent biopsy are critical for early definitive diagnosis and treatment, in order to prevent complications. Accumulating reports have revealed that EoE has several non-specific characteristic endoscopic findings, such as rings, furrows, white exudates, stricture/narrowing, edema, and crepe-paper esophagus. These findings were recently unified under the EoE endoscopic reference score (EREFS), which has been widely used as an objective, standard measurement for endoscopic EoE assessment. However, the diagnostic consistency of those findings among endoscopists is still inadequate, leading to underdiagnosis or misdiagnosis. Some endoscopic findings suggestive of EoE, such as multiple polypoid lesions, caterpillar sign, ankylosaurus back sign, and tug sign/pull sign, will aid the diagnosis. In addition, image-enhanced endoscopy represented by narrow band imaging, endocytoscopy, and artificial intelligence are expected to render endoscopic diagnosis more efficient and less invasive. This review focuses on suggestions for endoscopic assessment and biopsy, including recent advances in optical technology which may improve the diagnosis of EoE.
Keywords: EREFS scoring; diagnostic accuracy; endoscopic diagnosis; eosinophilic esophagitis; image enhanced endoscopy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Severity of endoscopically identified esophageal rings correlates with reduced esophageal distensibility in eosinophilic esophagitis.Endoscopy. 2016 Sep;48(9):794-801. doi: 10.1055/s-0042-107340. Epub 2016 May 20. Endoscopy. 2016. PMID: 27200524 Free PMC article.
-
The "caterpillar sign": a novel endoscopic indicator of eosinophilic esophagitis.Esophagus. 2021 Jan;18(1):156-162. doi: 10.1007/s10388-020-00791-0. Epub 2020 Oct 23. Esophagus. 2021. PMID: 33098035
-
Do endoscopic features suggesting eosinophilic esophagitis represent histological eosinophilia?Dig Endosc. 2014 Mar;26(2):156-63. doi: 10.1111/den.12091. Epub 2013 Apr 14. Dig Endosc. 2014. PMID: 23581603
-
The role of endoscopy in eosinophilic esophagitis: from diagnosis to therapy.Expert Rev Gastroenterol Hepatol. 2017 Dec;11(12):1135-1149. doi: 10.1080/17474124.2017.1367664. Epub 2017 Aug 17. Expert Rev Gastroenterol Hepatol. 2017. PMID: 28803528 Review.
-
Role of endoscopy in eosinophilic esophagitis.Clin Endosc. 2025 Jan;58(1):1-9. doi: 10.5946/ce.2024.023. Epub 2024 Jul 5. Clin Endosc. 2025. PMID: 38965710 Free PMC article. Review.
Cited by
-
Prevalence and Distribution of Gastric Endoscopy Findings in Non-eosinophilic Esophagitis Eosinophilic Gastrointestinal Diseases: Influence of Atrophic Gastritis.Intern Med. 2025 Apr 15;64(8):1161-1170. doi: 10.2169/internalmedicine.4193-24. Epub 2024 Sep 11. Intern Med. 2025. PMID: 39261065 Free PMC article.
-
Exploring the Link Between Atopic Dermatitis and Eosinophilic Esophagitis.J Clin Aesthet Dermatol. 2025 Mar;18(3):15-20. J Clin Aesthet Dermatol. 2025. PMID: 40135176 Free PMC article. Review.
-
Endoscopic Management of Eosinophilic Esophagitis: A Narrative Review on Diagnosis and Treatment.J Clin Med. 2025 May 27;14(11):3756. doi: 10.3390/jcm14113756. J Clin Med. 2025. PMID: 40507518 Free PMC article. Review.
-
Benralizumab treatment in an elderly patient with eosinophilic esophagitis resulted in remission: a case report.BMC Geriatr. 2024 Jan 24;24(1):92. doi: 10.1186/s12877-024-04683-1. BMC Geriatr. 2024. PMID: 38267847 Free PMC article.
-
Eosinophilic esophagitis: Current concepts in diagnosis and management.Saudi J Gastroenterol. 2024 Jul 1;30(4):210-227. doi: 10.4103/sjg.sjg_50_24. Epub 2024 May 16. Saudi J Gastroenterol. 2024. PMID: 38752302 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
