

Impact of X-Linked Hypophosphatemia on Muscle Symptoms
- PMID: 36553684
- PMCID: PMC9778127
- DOI: 10.3390/genes13122415
Impact of X-Linked Hypophosphatemia on Muscle Symptoms
Abstract
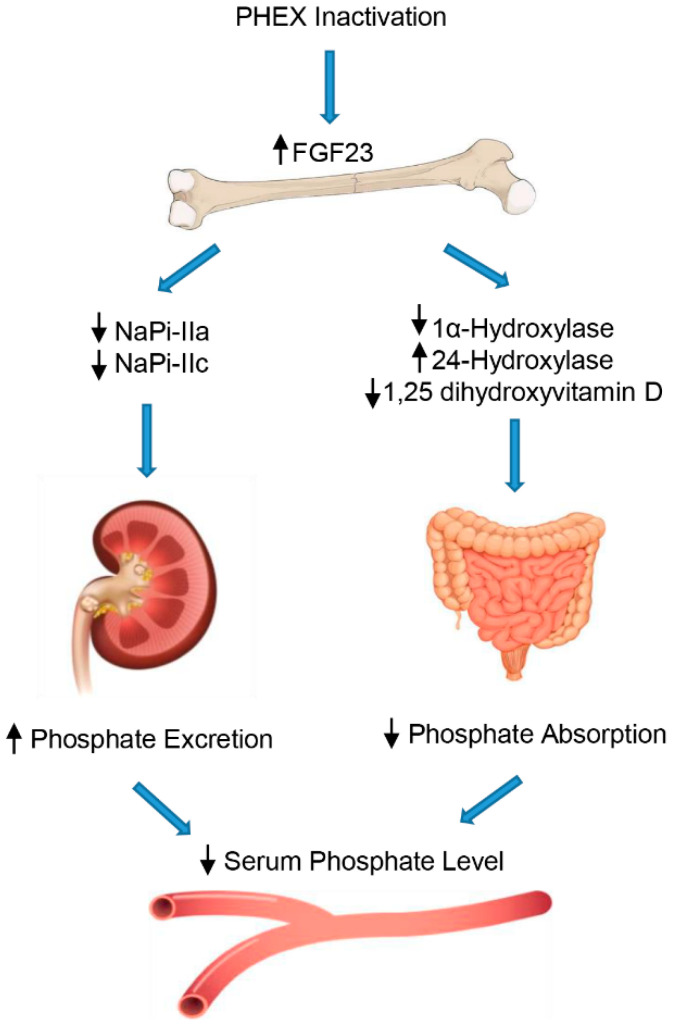
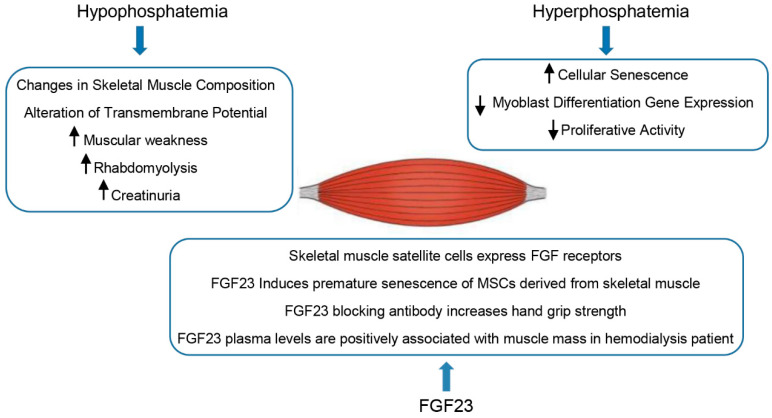
X-linked hypophosphatemia (XLH) is the most common hereditary form of rickets and deficiency of renal tubular phosphate transport in humans. XLH is caused by the inactivation of mutations within the phosphate-regulating endopeptidase homolog X-linked (PHEX) gene and follows an X-dominant transmission. It has an estimated frequency of 1 case per 20,000, and over 300 distinct pathogenic variations have been reported that result in an excess of fibroblast growth factor 23 (FGF23) in the serum. Increased levels of FGF23 lead to renal phosphate loss, decreased serum 1,25-dihydroxyvitamin D, and increased metabolism of 1,25-dihydoxyvitamin D, resulting in hypophosphatemia. Major clinical manifestations include rickets, bone deformities, and growth retardation that develop during childhood, and osteomalacia-related fractures or pseudo-fractures, degenerative osteoarthritis, enthesopathy, dental anomalies, and hearing loss during adulthood, which can affect quality of life. In addition, fatigue is also a common symptom in patients with XLH, who experience decreased motion, muscle weakness, and pain, contributing to altered quality of life. The clinical and biomedical characteristics of XLH are extensively defined in bone tissue since skeletal deformations and mineralization defects are the most evident effects of high FGF23 and low serum phosphate levels. However, despite the muscular symptoms that XLH causes, very few reports are available on the effects of FGF23 and phosphate in muscle tissue. Given the close relationship between bones and skeletal muscles, studying the effects of FGF23 and phosphate on muscle could provide additional opportunities to understand the interactions between these two important compartments of the body. By describing the current literature on XLH and skeletal muscle dysfunctions, the purpose of this review is to highlight future areas of research that could contribute to a better understanding of XLH muscular disability and its management.
Keywords: FGF23; X-linked hypophosphatemia; muscle weakness; skeletal muscle; skeletal muscle dysfunction.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Safety and efficacy of burosumab in improving phosphate metabolism, bone health, and quality of life in adolescents with X-linked hypophosphatemic rickets.Eur J Med Genet. 2024 Aug;70:104958. doi: 10.1016/j.ejmg.2024.104958. Epub 2024 Jun 29. Eur J Med Genet. 2024. PMID: 38950880
-
FGF23 and its role in X-linked hypophosphatemia-related morbidity.Orphanet J Rare Dis. 2019 Feb 26;14(1):58. doi: 10.1186/s13023-019-1014-8. Orphanet J Rare Dis. 2019. PMID: 30808384 Free PMC article. Review.
-
Diagnosis and management of X-linked hypophosphatemia in children and adolescent in the Gulf Cooperation Council countries.Arch Osteoporos. 2021 Mar 4;16(1):52. doi: 10.1007/s11657-021-00879-9. Arch Osteoporos. 2021. PMID: 33660084 Free PMC article.
-
Spectrum of PHEX Mutations and FGF23 Profiles in a Taiwanese Cohort With X-Linked Hypophosphatemia Including 102 Patients.In Vivo. 2024 Jan-Feb;38(1):341-350. doi: 10.21873/invivo.13444. In Vivo. 2024. Retraction in: In Vivo. 2024 Jul-Aug;38(4):2097. doi: 10.21873/invivo.13670. PMID: 38148081 Free PMC article. Retracted.
-
X-Linked Hypophosphatemia and FGF23-Related Hypophosphatemic Diseases: Prospect for New Treatment.Endocr Rev. 2018 Jun 1;39(3):274-291. doi: 10.1210/er.2017-00220. Endocr Rev. 2018. PMID: 29381780 Review.
Cited by
-
Mutational spectrum and phenotypic variability of Duchenne muscular dystrophy and related disorders in a Bangladeshi population.Sci Rep. 2023 Dec 6;13(1):21547. doi: 10.1038/s41598-023-48982-w. Sci Rep. 2023. PMID: 38057384 Free PMC article.
-
Prevalence of enthesopathies in X-linked hypophosphatemia: an explorative ultrasound study.JBMR Plus. 2025 Jul 7;9(9):ziaf113. doi: 10.1093/jbmrpl/ziaf113. eCollection 2025 Sep. JBMR Plus. 2025. PMID: 40800666 Free PMC article.
-
Role of transporters in regulating mammalian intracellular inorganic phosphate.Front Pharmacol. 2023 Mar 30;14:1163442. doi: 10.3389/fphar.2023.1163442. eCollection 2023. Front Pharmacol. 2023. PMID: 37063296 Free PMC article. Review.
-
Factors associated with impaired physical functionality in X-linked hypophosphatemia.JBMR Plus. 2025 Feb 2;9(4):ziaf018. doi: 10.1093/jbmrpl/ziaf018. eCollection 2025 Apr. JBMR Plus. 2025. PMID: 40092459
-
Effect of Burosumab on Muscle Function and Strength, and Rates of ATP Synthesis in Skeletal Muscle in Adults With XLH.J Clin Endocrinol Metab. 2024 Feb 20;109(3):e1061-e1071. doi: 10.1210/clinem/dgad642. J Clin Endocrinol Metab. 2024. PMID: 37930769 Free PMC article.
References
-
- Haffner D., Emma F., Eastwood D.M., Duplan M.B., Bacchetta J., Schnabel D., Wicart P., Bockenhauer D., Santos F., Levtchenko E., et al. Clinical practice recommendations for the diagnosis and management of X-linked hypophosphataemia. Nat. Rev. Nephrol. 2019;15:435–455. doi: 10.1038/s41581-019-0152-5. - DOI - PMC - PubMed
-
- Barros N.M.T., Hoac B., Neves R.L., Addison W.N., Assis D.M., Murshed M., Carmona A.K., McKee M.D. Proteolytic processing of osteopontin by PHEX and accumulation of osteopontin fragments in Hyp mouse bone, the murine model of X-linked hypophosphatemia. J. Bone Miner. Res. 2013;28:688–699. doi: 10.1002/jbmr.1766. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
