

Selective CB2 Receptor Agonist, HU-308, Reduces Systemic Inflammation in Endotoxin Model of Pneumonia-Induced Acute Lung Injury
- PMID: 36555499
- PMCID: PMC9779896
- DOI: 10.3390/ijms232415857
Selective CB2 Receptor Agonist, HU-308, Reduces Systemic Inflammation in Endotoxin Model of Pneumonia-Induced Acute Lung Injury
Abstract
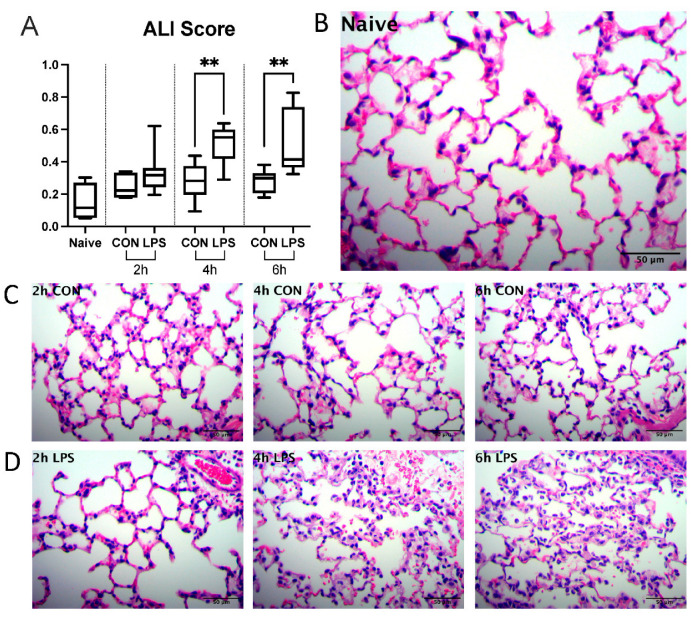
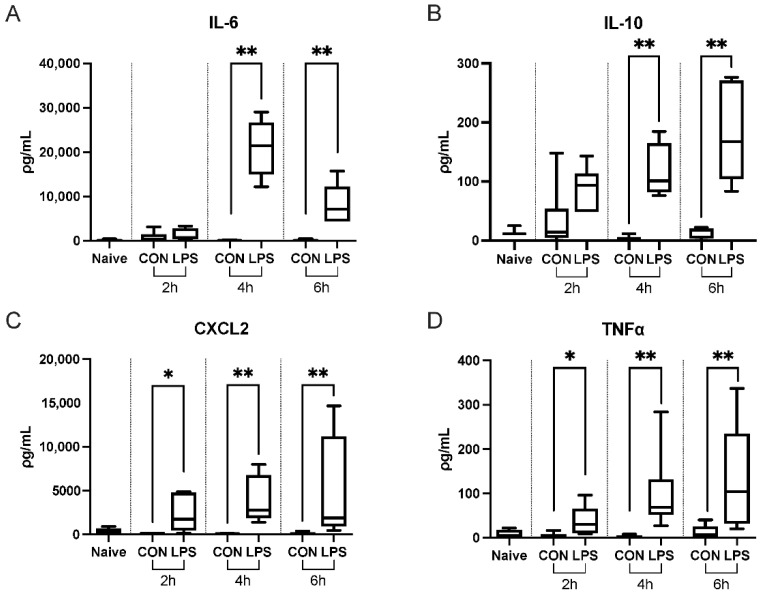
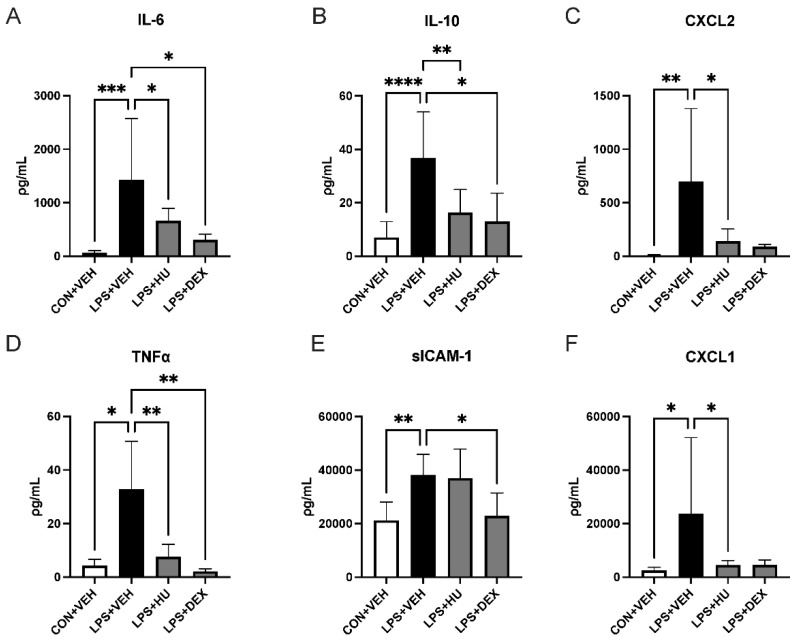
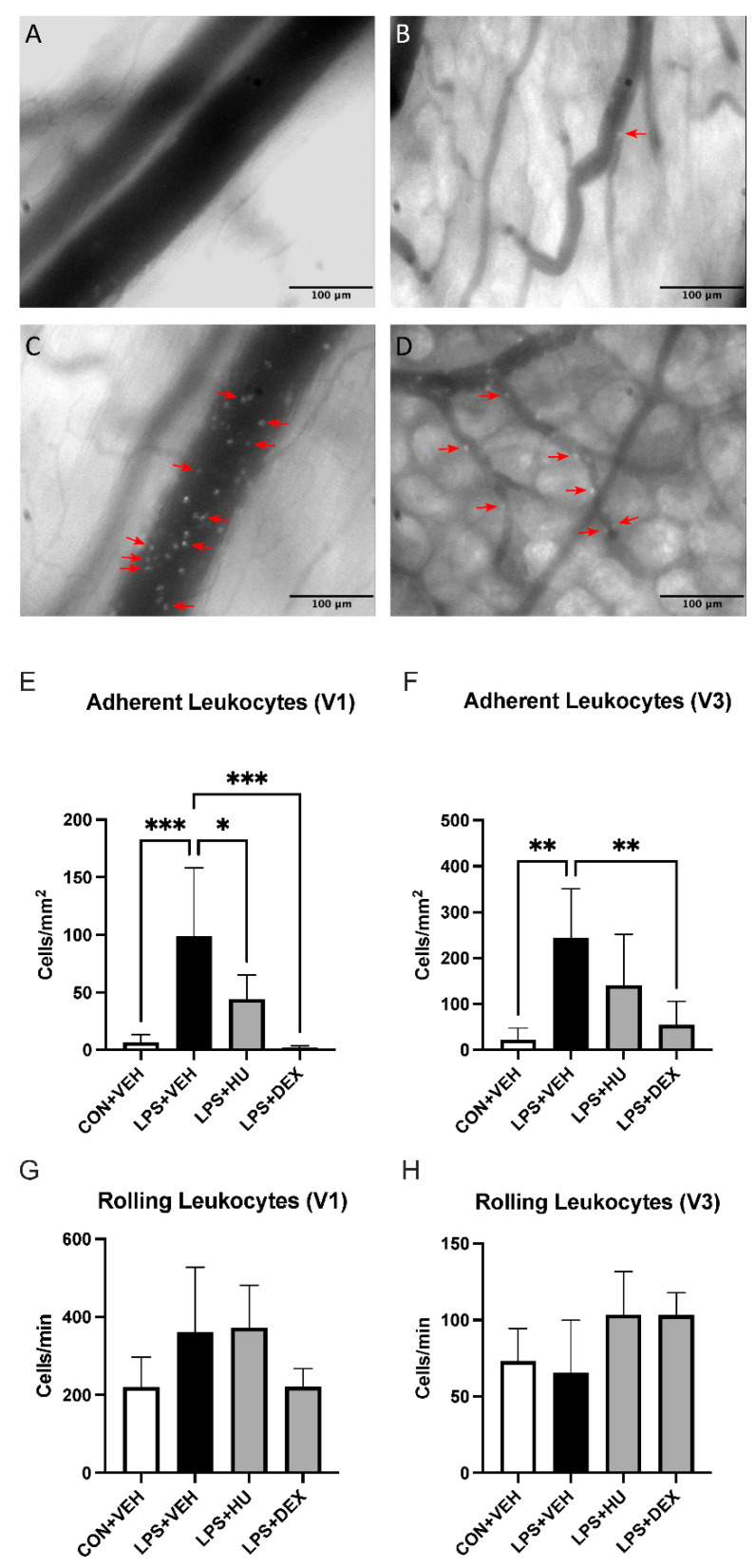
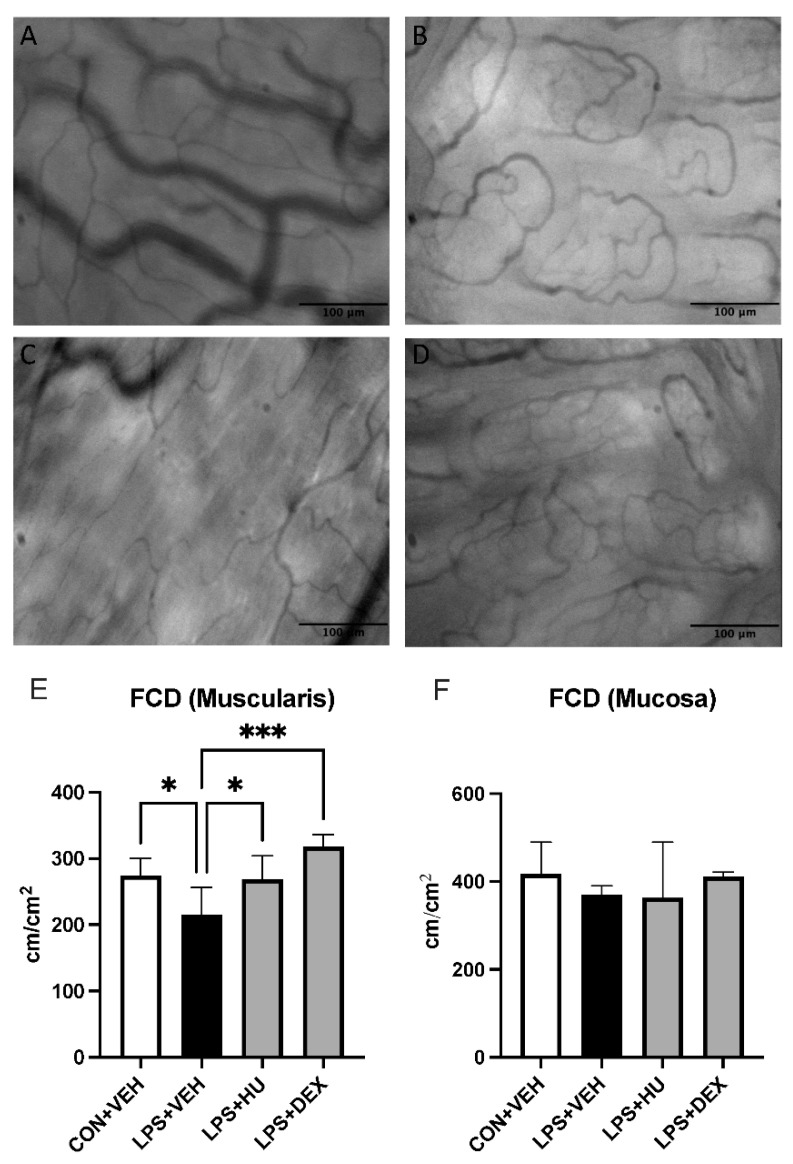
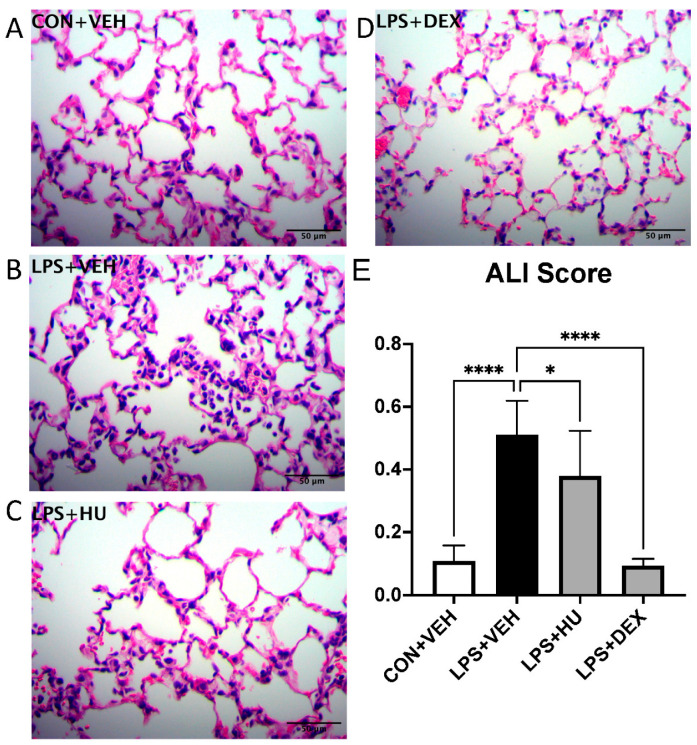
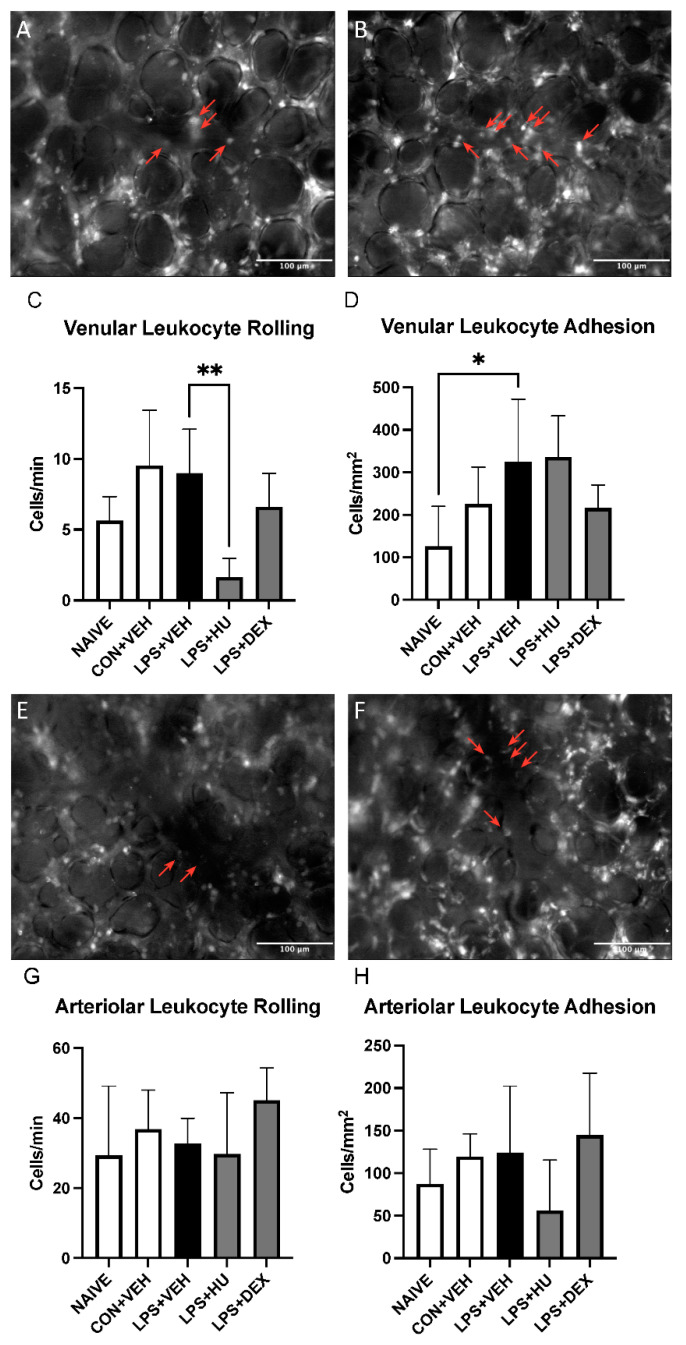
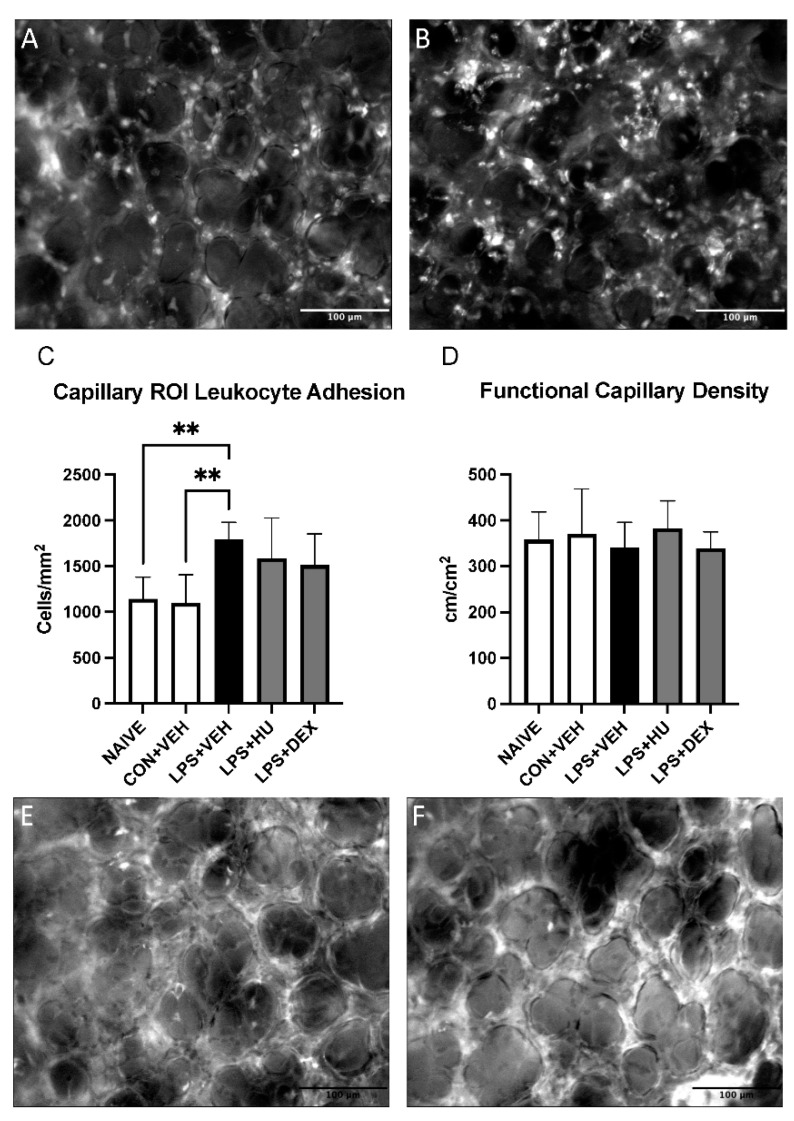
Acute respiratory distress syndrome (ARDS) and sepsis are risk factors contributing to mortality in patients with pneumonia. In ARDS, also termed acute lung injury (ALI), pulmonary immune responses lead to excessive pro-inflammatory cytokine release and aberrant alveolar neutrophil infiltration. Systemic spread of cytokines is associated with systemic complications including sepsis, multi-organ failure, and death. Thus, dampening pro-inflammatory cytokine release is a viable strategy to improve outcome. Activation of cannabinoid type II receptor (CB2) has been shown to reduce cytokine release in various in vivo and in vitro studies. Herein, we investigated the effect of HU-308, a specific CB2 agonist, on systemic and pulmonary inflammation in a model of pneumonia-induced ALI. C57Bl/6 mice received intranasal endotoxin or saline, followed by intravenous HU-308, dexamethasone, or vehicle. ALI was scored by histology and plasma levels of select inflammatory mediators were assessed by Luminex assay. Intravital microscopy (IVM) was performed to assess leukocyte adhesion and capillary perfusion in intestinal and pulmonary microcirculation. HU-308 and dexamethasone attenuated LPS-induced cytokine release and intestinal microcirculatory impairment. HU-308 modestly reduced ALI score, while dexamethasone abolished it. These results suggest administration of HU-308 can reduce systemic inflammation without suppressing pulmonary immune response in pneumonia-induced ALI and systemic inflammation.
Keywords: ARDS; acute lung injury; cannabinoid type II receptor (CB2); cytokines; inflammation; intravital microscopy; microcirculation.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Bellani G., Laffey J.G., Pham T., Fan E., Brochard L., Esteban A., Gattinoni L., Van Haren F.M.P., Larsson A., McAuley D.F., et al. Epidemiology, Patterns of Care, and Mortality for Patients with Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA—J. Am. Med. Assoc. 2016;315:788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
