

Stepwise Reduction of Mycophenolate Mofetil with Conversion to Everolimus for the Treatment of Active BKV in Kidney Transplant Recipients: A Single-Center Experience in Vietnam
- PMID: 36555914
- PMCID: PMC9783583
- DOI: 10.3390/jcm11247297
Stepwise Reduction of Mycophenolate Mofetil with Conversion to Everolimus for the Treatment of Active BKV in Kidney Transplant Recipients: A Single-Center Experience in Vietnam
Abstract
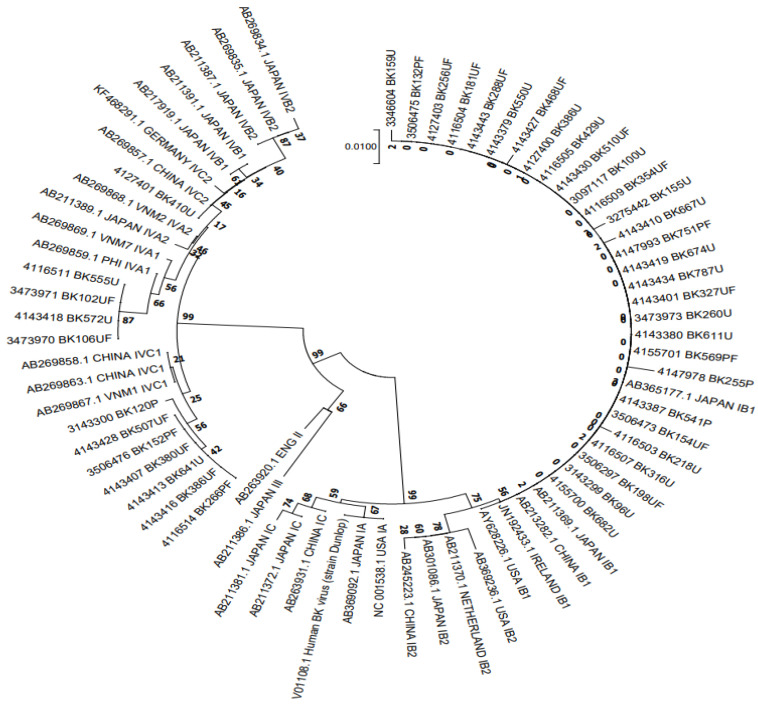
Background: No specific antiviral drug can effectively treat BKV reactivation after kidney transplantation. Thus, we evaluated stepwise-reduced immunosuppression to treat BKV reactivation. Methods: 341 kidney-transplant recipients were monitored for BKV infection (BKV-viremia, BKV-viruria). Positive samples with a significant virus load were nested PCR-genotyped in the VP1 region. In 97/211 patients presenting BKV viremia ≥104 copies/mL and/or BKV viruria ≥107 copies/mL, or BKV-nephropathy immunosuppression (i.e., mycophenolate mofetil [MMF]) was reduced by 50%. If viral load did not decrease within 28 days, MMF dose was further reduced by 25%, although calcineurin-inhibitor (CNI) therapy remained unchanged. If BKV viral load did not decrease within another 28 days, MMF was withdrawn and replaced by everolimus combined with reduced CNIs. Results: Only 41/97 BKV (+) cases completed the 6-month follow-up. Among these, 29 (71%) were in the BKV-I group and 12 (29%) were in BKV-IV. BKV viruria and BKV viremia were significantly decreased from 9.32 to 6.09 log10 copies/mL, and from 3.59 to 2.45 log10 copies/mL (p < 0.001 and p = 0.024, respectively). 11/32 (34.4%) patients were cleared of BKV viremia; 2/32 (6.3%) patients were cleared of BKV in both serum and urine, and 9/9 (100%) only had BKV viruria but did not develop BKV viremia. eGFR remained stable. No patient with BKV-related nephropathy had graft loss. There was a significant inverse relationship between changes in eGFR and serum BKV load (r = −0.314, p = 0.04). Conclusions: This stepwise immunosuppressive strategy proved effective at reducing BKV viral load in kidney transplant recipients that had high BKV loads in serum and/or urine. Renal function remained stable without rejection.
Keywords: BK polyomavirus; BKV genotypes; Vietnam; everolimus; immunosuppression; kidney transplantation; renal allograft rejection.
Conflict of interest statement
The authors declare no conflict of interest.
Figures




References
-
- Comerlato J., Campos F.S., Oliveira M.T., Cibulski S.P., Corrêa L., Kulmann M.I., Arantes T.S., Hentges L.P., Spilki F.R., Roehe P.M., et al. Molecular detection and characterization of BK and JC polyomaviruses in urine samples of renal transplant patients in Southern Brazil. J. Med. Virol. 2015;87:522–528. doi: 10.1002/jmv.24086. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
