

Spontaneous Breathing and Pendelluft in Patients with Acute Lung Injury: A Narrative Review
- PMID: 36556064
- PMCID: PMC9783194
- DOI: 10.3390/jcm11247449
Spontaneous Breathing and Pendelluft in Patients with Acute Lung Injury: A Narrative Review
Abstract
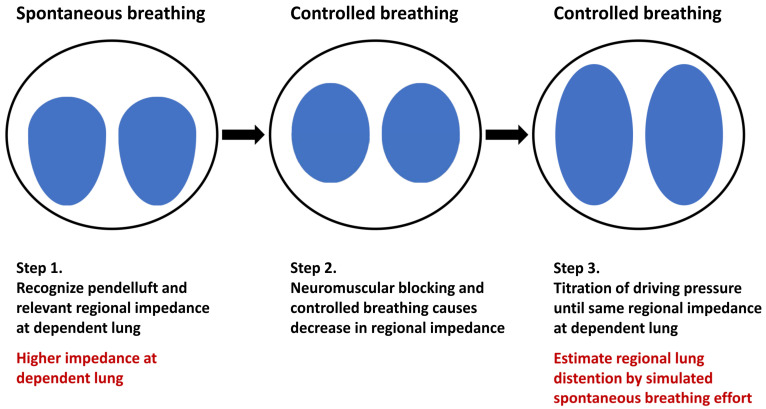
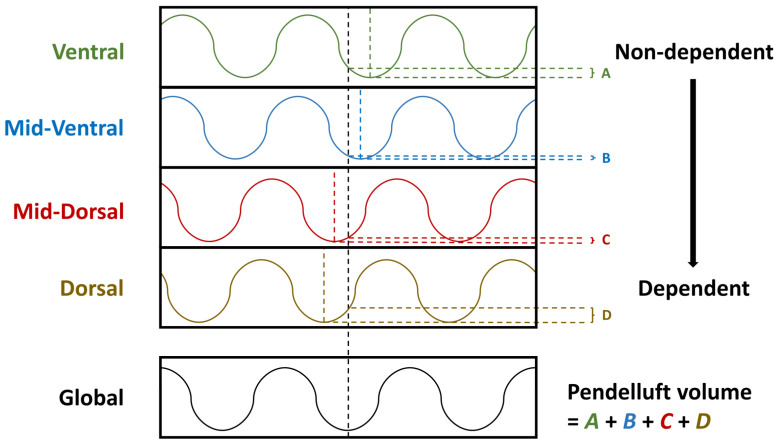
Acute respiratory distress syndrome (ARDS) is characterized by acute-onset rapid-deteriorating inflammatory lung injury. Although the preservation of spontaneous breathing may have physiological benefits in oxygenation, increasing evidence shows that vigorous spontaneous breathing may aggravate lung injury (i.e., patient self-inflicted lung injury). Increased lung stress and pendelluft, which is defined as intrapulmonary gas redistribution without a significant change in tidal volume, are important mechanisms of patient self-inflicted lung injury. The presence of pendelluft may be considered a surrogate marker of vigorous inspiratory effort, which can cause the dependent lung to overstretch. In this review, we summarized three major methods for electrical impedance tomography-based pendelluft monitoring. Future studies are warranted to compare and validate the different methods of pendelluft estimation in patients with ARDS.
Keywords: acute respiratory distress syndrome; pendelluft; spontaneous breathing.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Spontaneous Effort During Mechanical Ventilation: Maximal Injury With Less Positive End-Expiratory Pressure.Crit Care Med. 2016 Aug;44(8):e678-88. doi: 10.1097/CCM.0000000000001649. Crit Care Med. 2016. PMID: 27002273
-
Spontaneous effort causes occult pendelluft during mechanical ventilation.Am J Respir Crit Care Med. 2013 Dec 15;188(12):1420-7. doi: 10.1164/rccm.201303-0539OC. Am J Respir Crit Care Med. 2013. PMID: 24199628
-
Effect of Higher or Lower PEEP on Pendelluft During Spontaneous Breathing Efforts in Acute Hypoxemic Respiratory Failure.Respir Care. 2025 Feb;70(2):126-133. doi: 10.1089/respcare.12193. Respir Care. 2025. PMID: 39964850 Clinical Trial.
-
The role of spontaneous effort during mechanical ventilation: normal lung versus injured lung.J Intensive Care. 2015 Jun 17;3:18. doi: 10.1186/s40560-015-0083-6. eCollection 2015. J Intensive Care. 2015. PMID: 27408729 Free PMC article. Review.
-
Patient self-inflicted lung injury: implications for acute hypoxemic respiratory failure and ARDS patients on non-invasive support.Minerva Anestesiol. 2019 Sep;85(9):1014-1023. doi: 10.23736/S0375-9393.19.13418-9. Epub 2019 Mar 12. Minerva Anestesiol. 2019. PMID: 30871304 Review.
Cited by
-
Hiccup-like Contractions in Mechanically Ventilated Patients: Individualized Treatment Guided by Transpulmonary Pressure.J Pers Med. 2023 Jun 12;13(6):984. doi: 10.3390/jpm13060984. J Pers Med. 2023. PMID: 37373973 Free PMC article.
-
Pendelluft in patients with acute respiratory distress syndrome during trigger and reverse triggering breaths.Sci Rep. 2023 Dec 13;13(1):22143. doi: 10.1038/s41598-023-49038-9. Sci Rep. 2023. PMID: 38092775 Free PMC article.
-
Occurrence of pendelluft during ventilator weaning with T piece correlated with increased mortality in difficult-to-wean patients.J Intensive Care. 2024 Jun 24;12(1):23. doi: 10.1186/s40560-024-00737-z. J Intensive Care. 2024. PMID: 38915067 Free PMC article.
-
The effect of target transpulmonary driving pressure values on mortality in ARDS patients: A retrospective study based on the MIMIC-IV database.PLoS One. 2025 Jun 18;20(6):e0326060. doi: 10.1371/journal.pone.0326060. eCollection 2025. PLoS One. 2025. PMID: 40531833 Free PMC article.
References
-
- Bellani G., Laffey J.G., Pham T., Fan E., Brochard L., Esteban A., Gattinoni L., van Haren F., Larsson A., McAuley D.F., et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315:788–800. doi: 10.1001/jama.2016.0291. - DOI - PubMed
-
- Fredericks A.S., Bunker M.P., Gliga L.A., Ebeling C.G., Ringqvist J.R., Heravi H., Manley J., Valladares J., Romito B.T. Airway pressure release ventilation: A review of the evidence, theoretical benefits, and alternative titration strategies. Clin. Med. Insights Circ. Respir. Pulm. Med. 2020;14:1179548420903297. doi: 10.1177/1179548420903297. - DOI - PMC - PubMed
-
- Carvalho A.R., Spieth P.M., Pelosi P., Beda A., Lopes A.J., Neykova B., Heller A.R., Koch T., Gama de Abreu M. Pressure support ventilation and biphasic positive airway pressure improve oxygenation by redistribution of pulmonary blood flow. Anesth. Analg. 2009;109:856–865. doi: 10.1213/ane.0b013e3181aff245. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
