

Answering Clinical Questions Using Machine Learning: Should We Look at Diastolic Blood Pressure When Tailoring Blood Pressure Control?
- PMID: 36556072
- PMCID: PMC9785044
- DOI: 10.3390/jcm11247454
Answering Clinical Questions Using Machine Learning: Should We Look at Diastolic Blood Pressure When Tailoring Blood Pressure Control?
Abstract
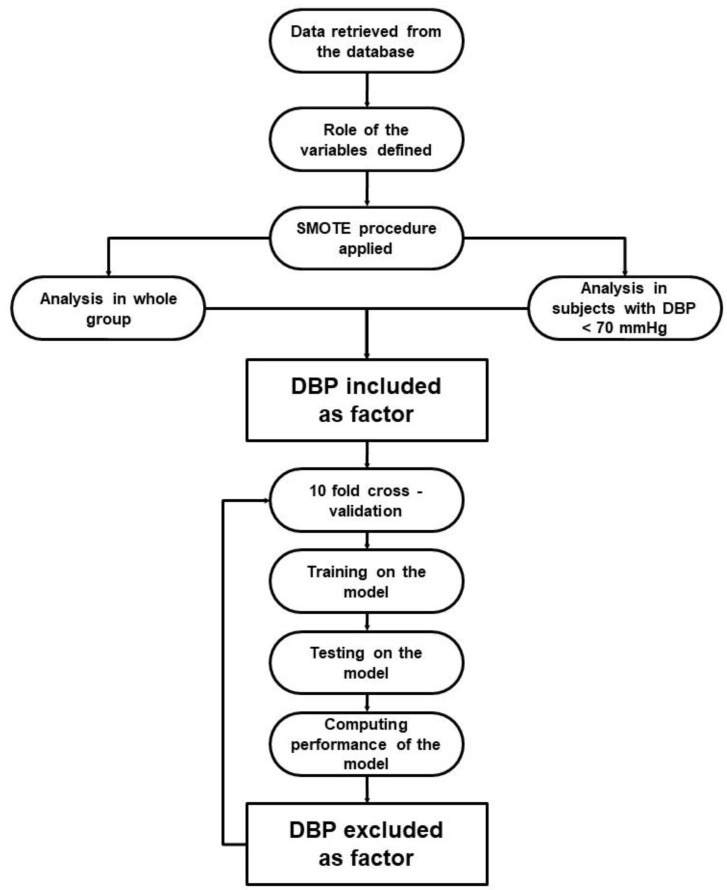
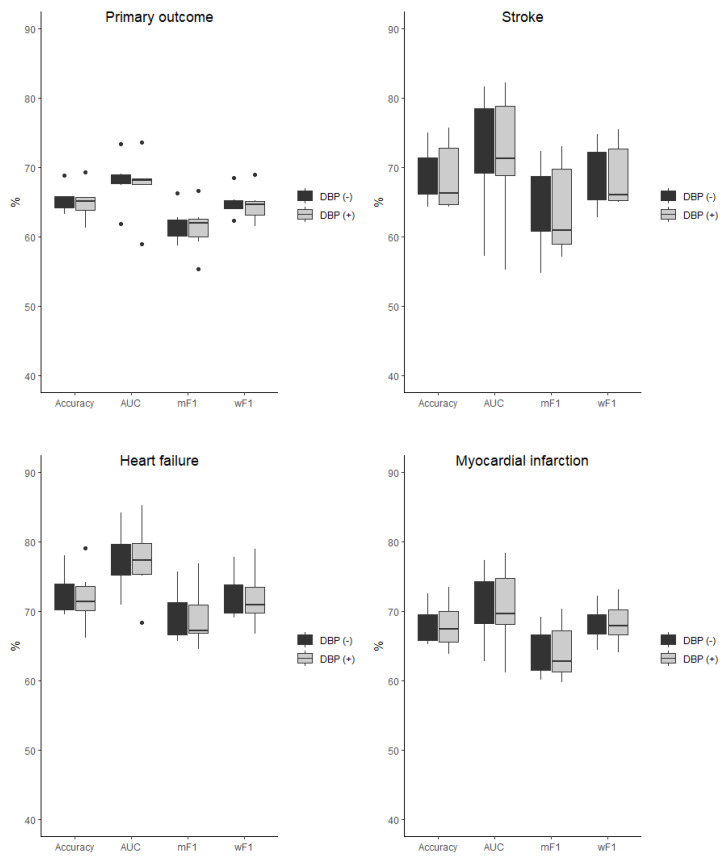
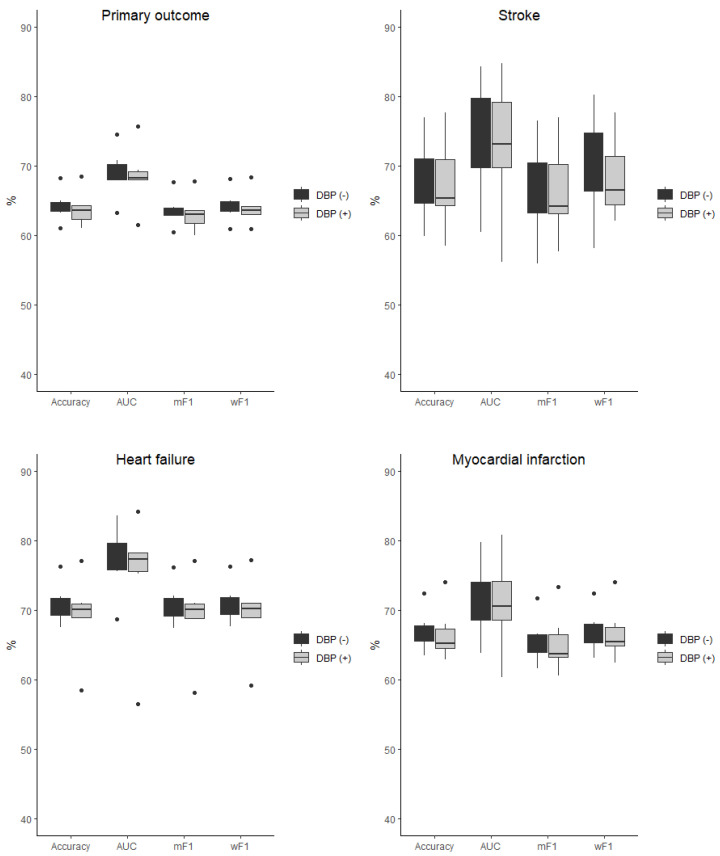
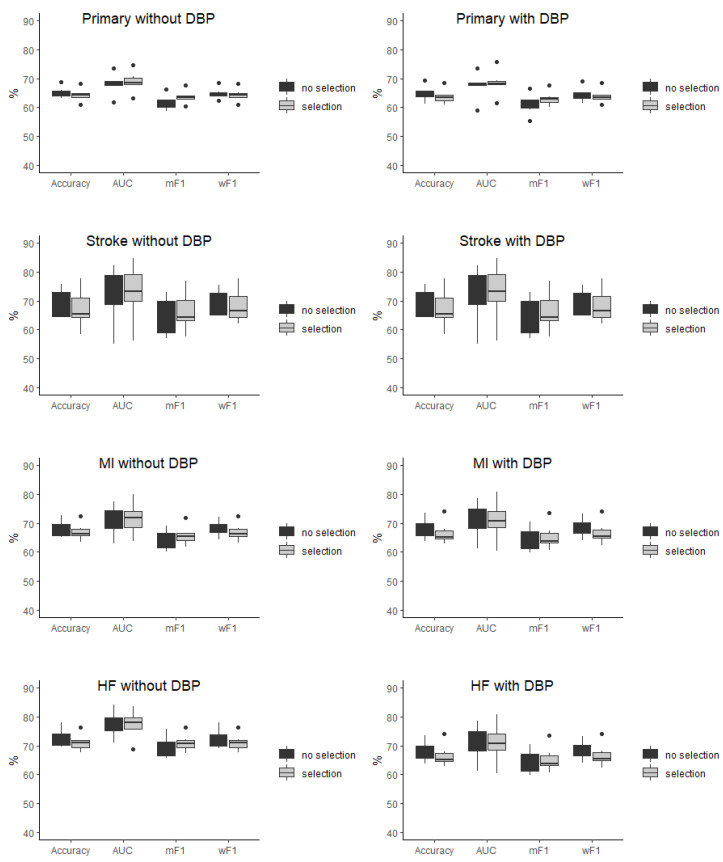
Background: The guidelines recommend intensive blood pressure control. Randomized trials have focused on the relevance of the systolic blood pressure (SBP) lowering, leaving the safety of the diastolic blood pressure (DBP) reduction unresolved. There are data available which show that low DBP should not stop clinicians from achieving SBP targets; however, registries and analyses of randomized trials present conflicting results. The purpose of the study was to apply machine learning (ML) algorithms to determine, whether DBP is an important risk factor to predict stroke, heart failure (HF), myocardial infarction (MI), and primary outcome in the SPRINT trial database. Methods: ML experiments were performed using decision tree, random forest, k-nearest neighbor, naive Bayesian, multi-layer perceptron, and logistic regression algorithms, including and excluding DBP as the risk factor in an unselected and selected (DBP < 70 mmHg) study population. Results: Including DBP as the risk factor did not change the performance of the machine learning models evaluated using accuracy, AUC, mean, and weighted F-measure, and was not required to make proper predictions of stroke, MI, HF, and primary outcome. Conclusions: Analyses of the SPRINT trial data using ML algorithms imply that DBP should not be treated as an independent risk factor when intensifying blood pressure control.
Keywords: SPRINT trial; cardiovascular risk; diastolic blood pressure; machine learning.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
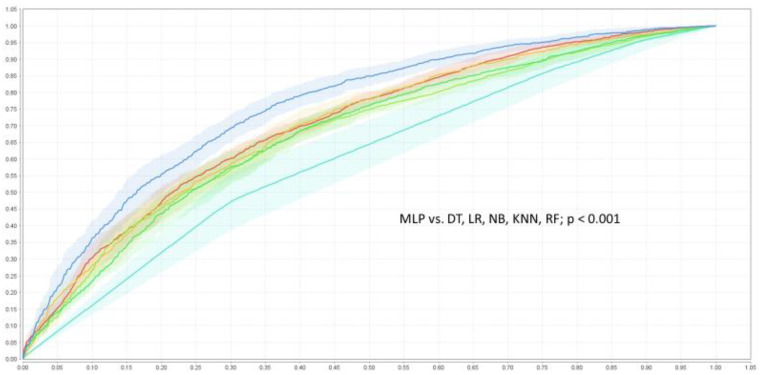
 , KNN—k-nearest neighbor classifier
, KNN—k-nearest neighbor classifier  , LR—logistic regression
, LR—logistic regression  , MLP—multi-layer perceptron
, MLP—multi-layer perceptron  , NB—naive Bayesian classifier
, NB—naive Bayesian classifier  , RF—random forest
, RF—random forest  .
.Similar articles
-
Contributions of Systolic and Diastolic Blood Pressures to Cardiovascular Outcomes in the ALLHAT Study.J Am Coll Cardiol. 2021 Oct 26;78(17):1671-1678. doi: 10.1016/j.jacc.2021.08.035. J Am Coll Cardiol. 2021. PMID: 34674811
-
Clinical benefit of systolic blood pressure within the target range among patients with or without diabetes mellitus: a propensity score-matched analysis of two randomized clinical trials.BMC Med. 2022 Jun 20;20(1):208. doi: 10.1186/s12916-022-02407-z. BMC Med. 2022. PMID: 35718771 Free PMC article.
-
Influence of Baseline Diastolic Blood Pressure on Effects of Intensive Compared With Standard Blood Pressure Control.Circulation. 2018 Jan 9;137(2):134-143. doi: 10.1161/CIRCULATIONAHA.117.030848. Epub 2017 Oct 11. Circulation. 2018. PMID: 29021322 Free PMC article. Clinical Trial.
-
Effects of blood pressure lowering on outcome incidence in hypertension: 2. Effects at different baseline and achieved blood pressure levels--overview and meta-analyses of randomized trials.J Hypertens. 2014 Dec;32(12):2296-304. doi: 10.1097/HJH.0000000000000379. J Hypertens. 2014. PMID: 25259547 Review.
-
Blood pressure targets in adults with hypertension.Cochrane Database Syst Rev. 2020 Dec 17;12(12):CD004349. doi: 10.1002/14651858.CD004349.pub3. Cochrane Database Syst Rev. 2020. PMID: 33332584 Free PMC article.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
