

Life Quality in Premenopausal Women after Embolization of Uterine Myomas
- PMID: 36556210
- PMCID: PMC9786225
- DOI: 10.3390/jpm12121990
Life Quality in Premenopausal Women after Embolization of Uterine Myomas
Abstract
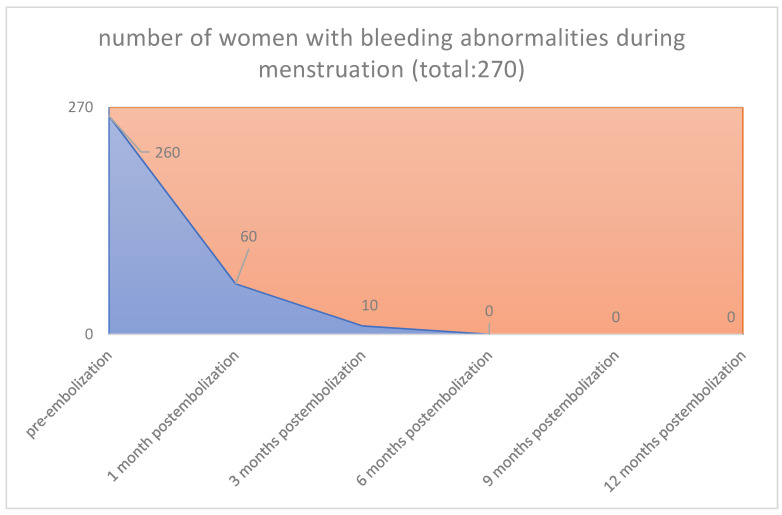
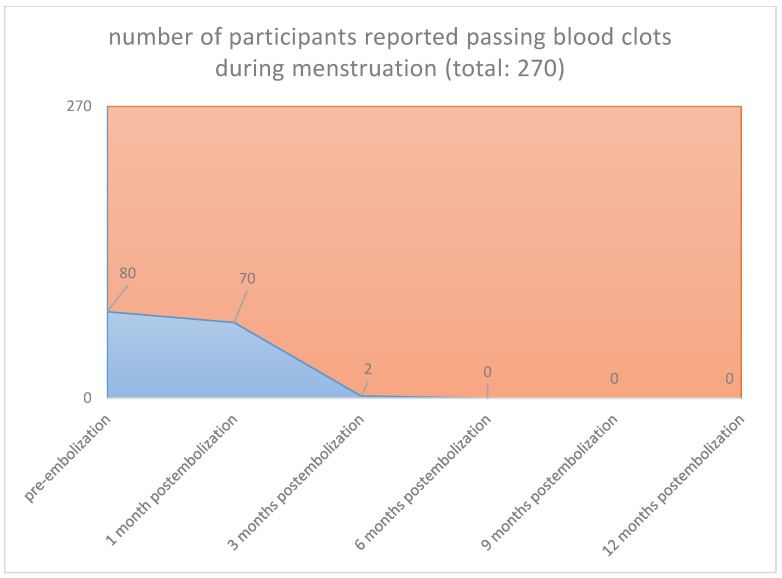
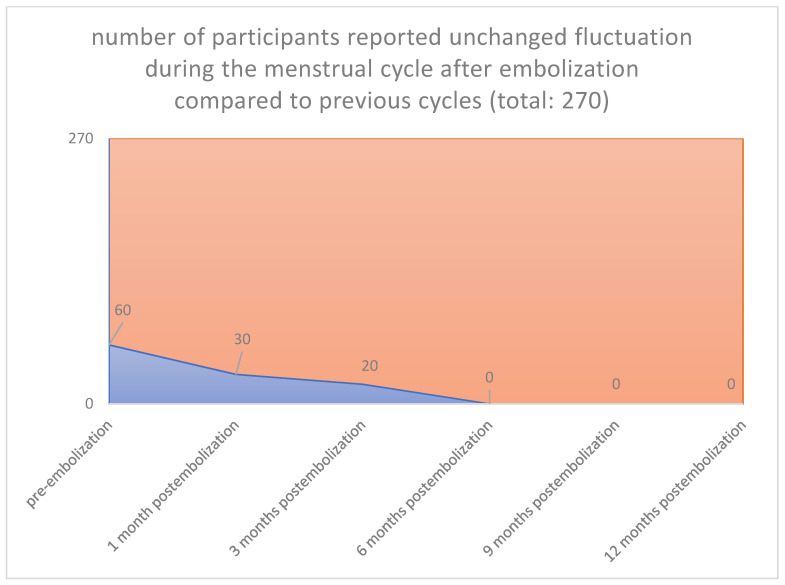
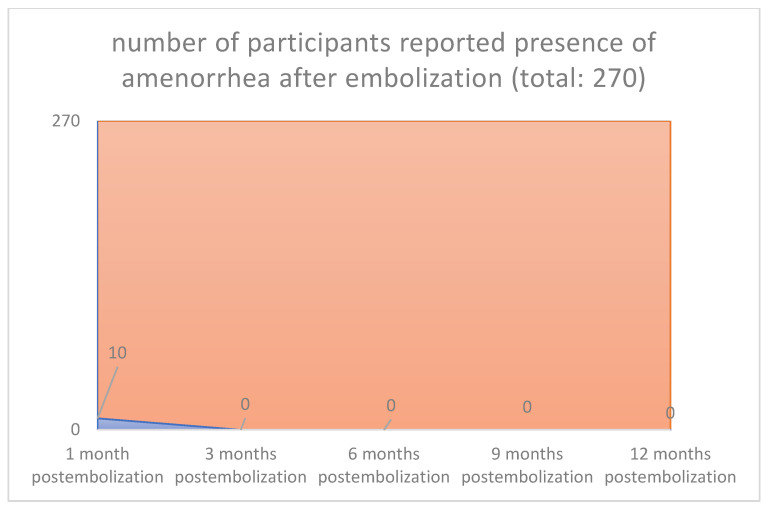
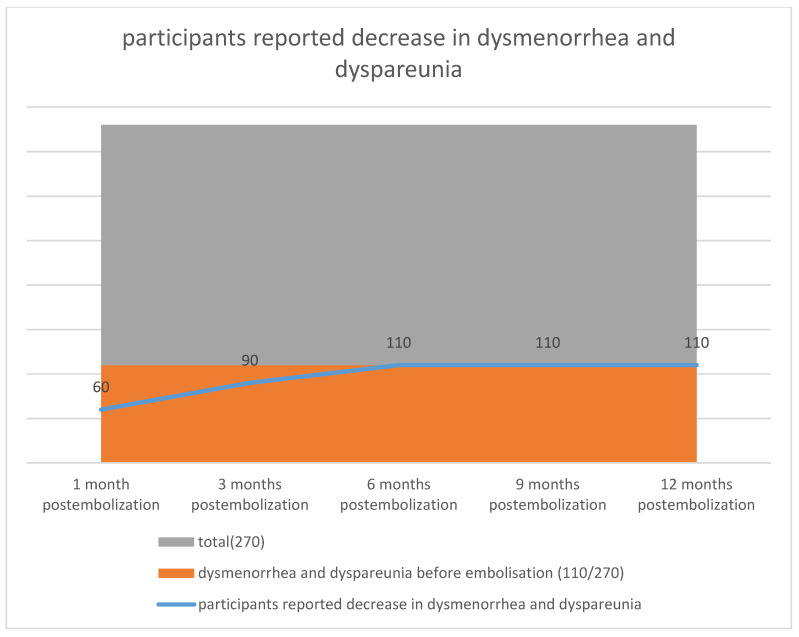
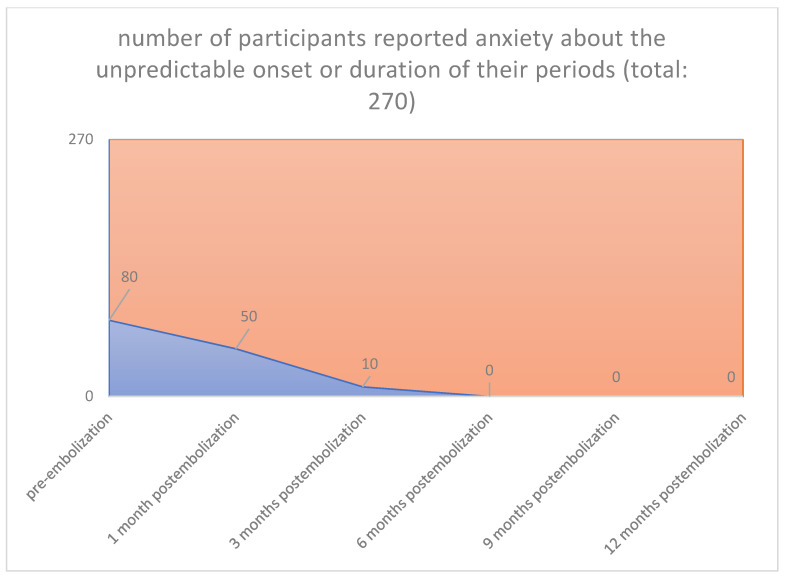
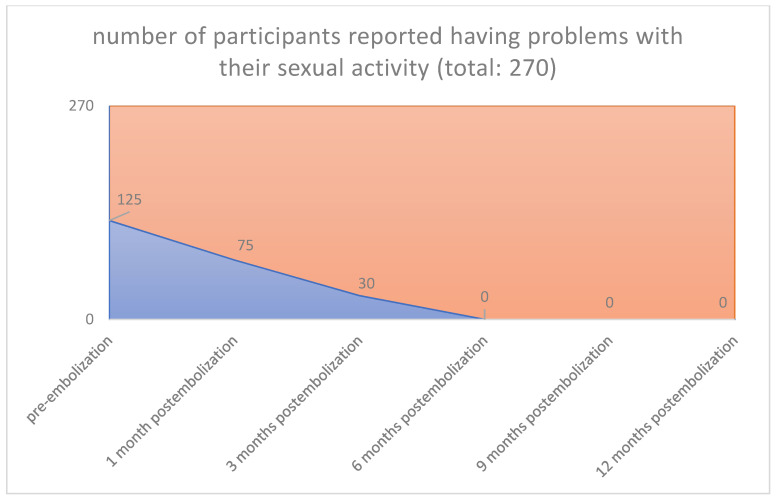
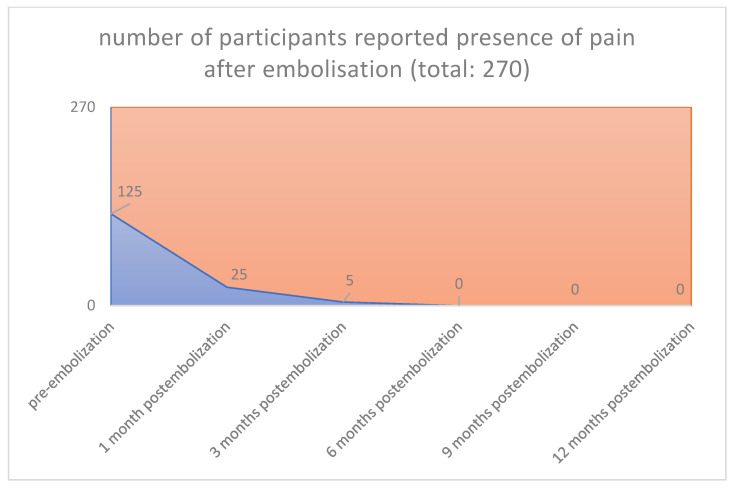
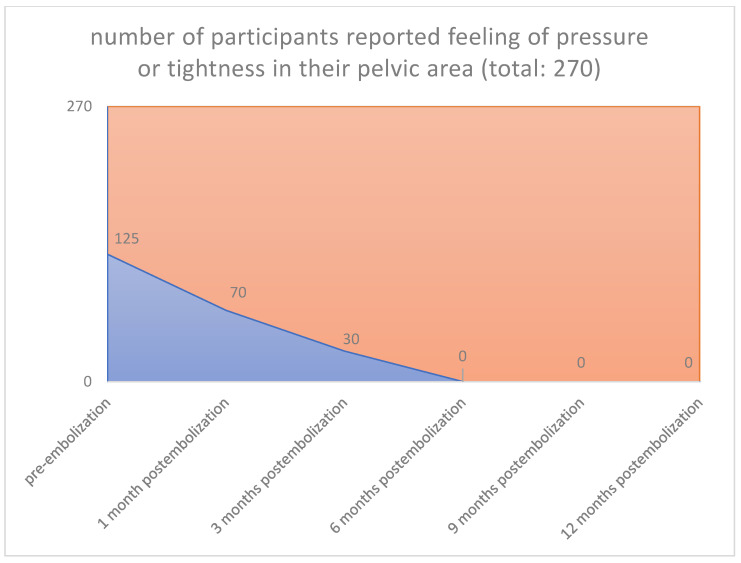
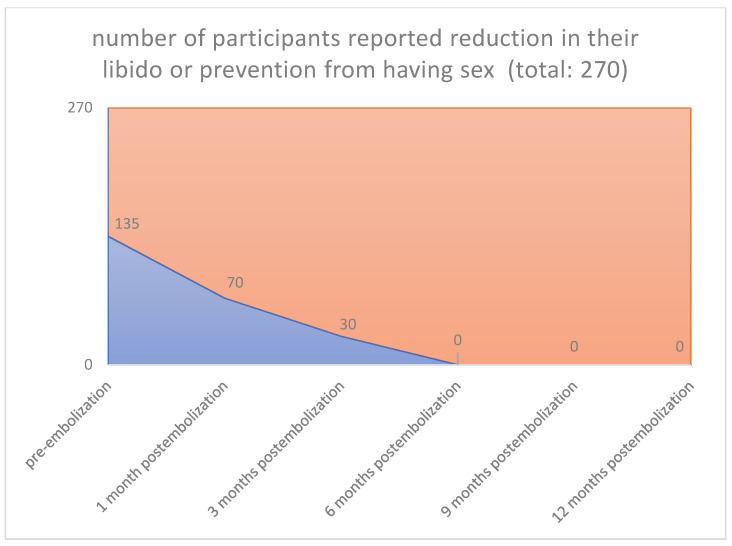
Objectives: Fibroids cause significant morbidity and are the most common indication for hysterectomies worldwide, delimiting a major public health problem. Uterine artery embolization (UAE) is an alternative therapy to surgical treatment of symptomatic fibroids; it has satisfactory long-time results and is no longer considered investigational for the treatment of symptomatic fibroids. This study was undertaken to evaluate changes in fibroid specific symptom severity and health-related quality of life (HRQOL) after UAE and to optimize the assessment of safety and outcomes measures for participants who receive UAE to objective compare UAE and surgical alternatives for therapy of symptomatic fibroids. Study design: The analysis was based on questionnaires completed by 270 pre-menopausal females with a mean age of 42 years (range, 38-50 years) who underwent UAE for uterine leiomyomas and/or adenomyosis from November 2013 through December 2019. Only symptomatic women were selected whose symptoms were not improving with medication and who did not wish to have children. The primary outcome measure was a change in fibroid symptoms and HRQOL (health related quality of life) after UAE. Secondary outcomes included the decrease in uterine volume after UAE. Results: Questionnaires were completed by 270 women (100%) at a mean of 12.1 months from UAE. The median follow-up period was two years. Uterine fibroid embolization led to a shrinkage at three months for the 90% of the participants. A reduction of bleeding symptoms, pain and bulk-related symptoms was observed in 89.7%, 88.9%, and 89.5% of the patients, respectively. In the long term, there was no significant difference in parameters assessed compared with the midterm follow-up findings. A total of 6 patients (2.3%) underwent fractional curettage an average of 32.1 months after intervention due to necrotic changes in submucosal fibroids. All participants continued to be satisfied with the intervention, and 240 patients (88.9%) answered that they would recommend uterine fibroid embolization to other patients. Conclusions: Women who undergo UAE have a significant decrease in symptom severity and increase in HRQOL which is associated with high levels of satisfaction with the procedure (even when subsequent therapies are pursued).
Keywords: life quality; premenopausal women; uterine artery embolization; uterine fibroids.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
