

Prognostic Impact of Different Types of Ventricular Tachyarrhythmias Stratified by Underlying Cardiac Disease
- PMID: 36556245
- PMCID: PMC9784877
- DOI: 10.3390/jpm12122023
Prognostic Impact of Different Types of Ventricular Tachyarrhythmias Stratified by Underlying Cardiac Disease
Abstract
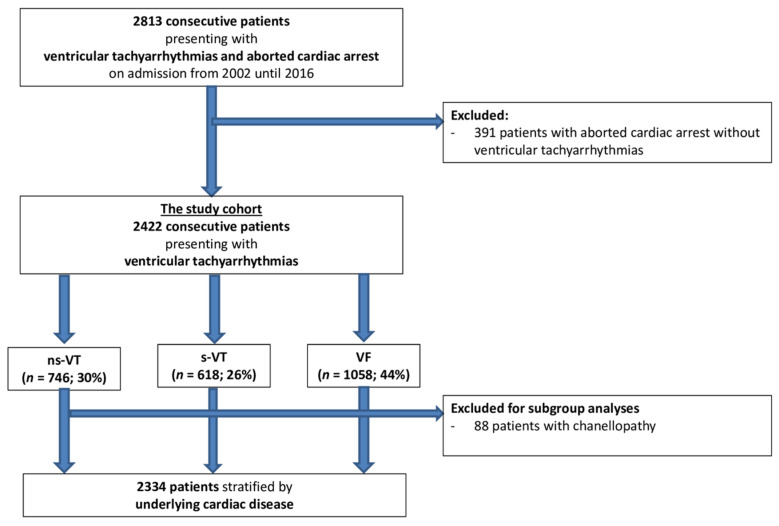
Limited data regarding the outcome of patients with different types of ventricular tachyarrhythmias is available. This study sought to assess the prognostic impact of different types of ventricular tachyarrhythmias stratified by underlying cardiac disease. A large retrospective registry was used including all consecutive patients presenting with ventricular tachycardia (VT) and fibrillation (VF) on admission from 2002 to 2016. Patients with non-sustained VT (ns-VT), sustained VT (s-VT) and VF were compared using uni- and multivariable Cox regression models. Risk stratification was performed after stratification by underlying cardiac disease (i.e., acute myocardial infarction (AMI), ischemic heart disease (IHD), non-ischemic cardiomyopathy (NICM) and patients considered as lower-risk for ventricular tachyarrhythmias). The primary endpoint was defined as all-cause mortality at 2.5 years. Secondary endpoints were cardiac death at 24 h, all-cause mortality at 5 years, cardiac rehospitalization and a composite arrhythmic endpoint at 2.5 years. In 2422 consecutive patients with ventricular tachyarrhythmias, most patients were admitted with VF (44%), followed by ns-VT (30%) and s-VT (26%). Patients with VF suffered most commonly from AMI (42%), whereas heart failure was more common in s-VT patients (32%). In patients with AMI (HR = 1.146; 95% CI 0.751-1.750; p = 0.527) and in the lower-risk group (HR = 1.357; 95% CI 0.702-2.625; p = 0.364), the risk of all-cause mortality did not differ in VF and s-VT patients. In IHD patients, VF was associated with impaired prognosis compared to s-VT (HR = 2.502; 95% CI 1.936-3.235; p = 0.001). In conclusion, VF was associated with worse long-term prognosis compared to s-VT in IHD patients, whereas the risk of all-cause mortality among VF and s-VT patients did not differ in patients with AMI, NICM and in patients considered at lower risk for ventricular tachyarrhythmias.
Keywords: mortality; sudden cardiac death; ventricular fibrillation; ventricular tachyarrhythmia; ventricular tachycardia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures





References
-
- Zeppenfeld K., Tfelt-Hansen J., de Riva M., Winkel B.G., Behr E.R., Blom N.A., Charron P., Corrado D., Dagres N., de Chillou C., et al. 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Eur. Heart J. 2022;43:3997–4126. doi: 10.1093/eurheartj/ehac262. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
