

The Effect of Low Doses of Acetylsalicylic Acid on the Occurrence of Rectal Aberrant Crypt Foci
- PMID: 36556972
- PMCID: PMC9788241
- DOI: 10.3390/medicina58121767
The Effect of Low Doses of Acetylsalicylic Acid on the Occurrence of Rectal Aberrant Crypt Foci
Abstract
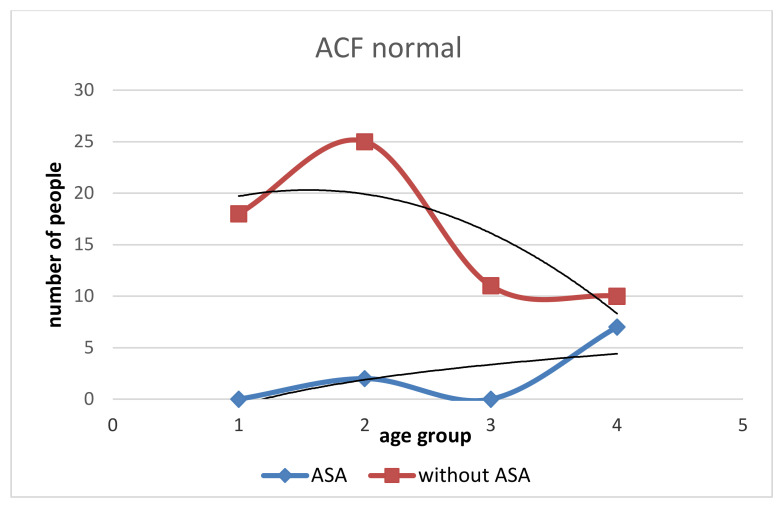
Background and Objectives: Aberrant crypt foci (ACF) are one of the earliest putative preneoplastic and, in some cases, neoplastic lesions in human colons. Many studies have confirmed the reduction of ACFs and colorectal adenomas after treatment with acetylsalicylic acid (ASA) commonly referred to as ASA; however, the minimum effective dose of ASA and the duration of use has not been fully elucidated. The objective of our study was to assess the significance of low dose ASA (75-mg internally once daily) to study the chemopreventive effect of ASA in ACF and adenomas development in patients taking this drug for a minimum period of 10 years. Materials and Methods: Colonoscopy, combined with rectal mucosa staining with 0.25% methylene blue, was performed on 131 patients. The number of rectal ACF in the colon was divided into three groups: ACF < 5; ACF 5−10; and ACF > 10. Patients were divided into two groups: the “With ASA” group (the study group subjects taking ASA 75-mg daily for 10 years); and “Without ASA” group (control group subjects not taking ASA chronically). The incidence of different types of rectal ACF and colorectal polyps in both groups of subjects was analysed and ascertained. Results: Normal ACF was found in 12.3% in the study group vs. 87.7% control group, hyperplastic 22.4% vs. 77.6%, dysplastic 25% vs. 75%, mixed 0% vs. 100%. Treatment with ASA affects the occurrence of colorectal adenomas. The amount of dysplastic ACFs was lower in the study group than in the control group. The increase in dysplastic ACFs decreases with age in both groups, with the increase greater in those not taking ASA. Conclusions: Patients who take persistent, chronic (>10 years) low doses of ASA have a lower total number of all types of rectal ACFs and adenomas compared to the control group.
Keywords: acetylsalicylic acid (ASA); colonoscopy; colorectal adenoma; colorectal cancer (CRC); rectal aberrant crypt foci (ACF).
Conflict of interest statement
The authors declare no conflict of interest.
Figures







References
-
- Cancer Stat Facts: Colorectal Cancer. [(accessed on 1 September 2022)]; Available online: https://seer.cancer.gov/statfacts/html/colorect.html.
-
- Benamouzig R., Deyra J., Martin A., Girard B., Jullian E., Piednoir B., Couturier D., Coste T., Little J., Chaussade S. Daily soluble aspirin and prevention of colorectal adenoma recurrence: One-year results of the APACC trial. Gastroenterology. 2003;125:328–336. doi: 10.1016/S0016-5085(03)00887-4. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
