

Exome Sequencing Revealed a Novel Splice Site Variant in the CRB2 Gene Underlying Nephrotic Syndrome
- PMID: 36556986
- PMCID: PMC9781877
- DOI: 10.3390/medicina58121784
Exome Sequencing Revealed a Novel Splice Site Variant in the CRB2 Gene Underlying Nephrotic Syndrome
Abstract
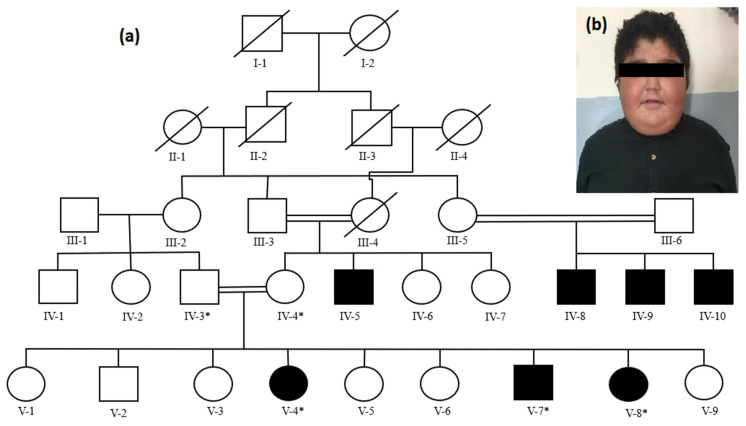
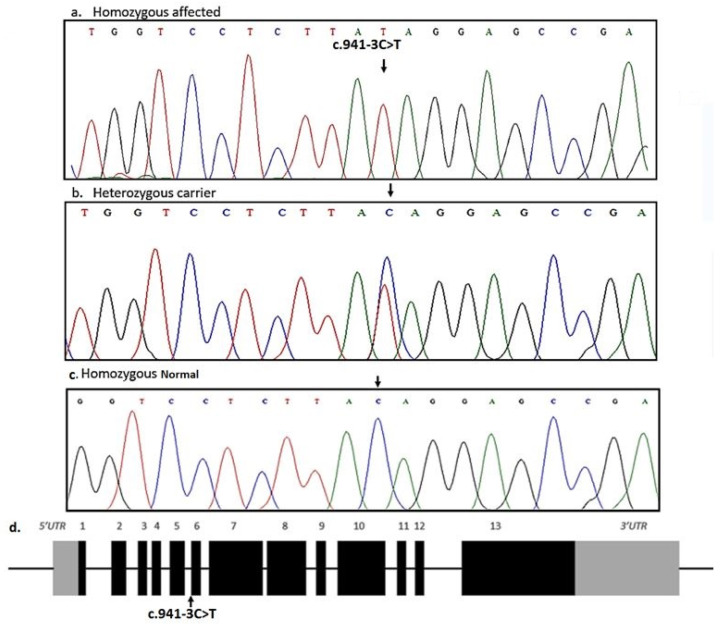
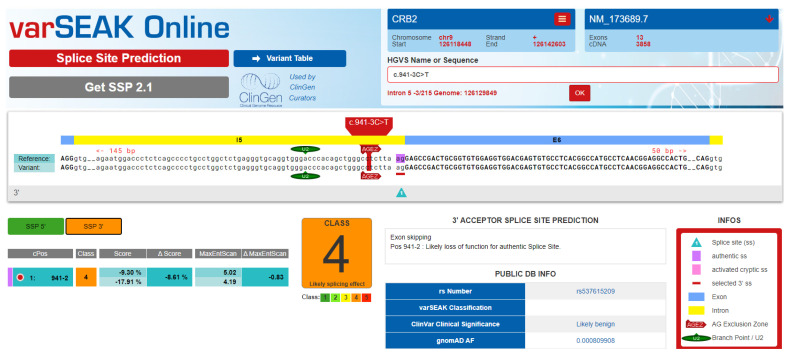
Background and Objectives: Nephrotic syndrome (NS) is a kidney disease where the patient has a classic triad of signs and symptoms including hypercholesterolemia, hypoalbuminemia, proteinuria (>3.5 g/24 h), and peripheral edema. In case of NS, the damaged nephrons (structural and functional unit of the kidney) filter unwanted blood contents to make urine. Thus, the urine contains unwanted proteins (proteinuria) and blood cells (hematuria), while the bloodstream lacks enough protein albumin (hypoalbuminemia). Nephrotic syndrome is divided into two types, primary NS, and secondary NS. Primary NS, also known as primary glomerulonephrosis, is the result of a glomerular disease that is limited to the kidney, while secondary NS is a condition that affects the kidney and other parts of the body. The main causes of primary NS are minimal change disease, membranous glomerulonephritis, and focal segmental glomerulosclerosis. In the present study we recruited a family segregating primary NS with the aim to identify the underlying genetic etiology. Such type of study is important in children because it allows counseling of other family members who may be at risk of developing NS, predicts risk of recurrent disease phenotypes after kidney transplant, and predicts response to immunosuppressive therapy. Materials and Methods: All affected individuals were clinically evaluated. Clinical examination, results of laboratory tests, and biopsy investigations led us to the diagnosis. The next-generation sequencing technique (whole-exome sequencing) followed by Sanger sequencing identified a novel homozygous splice site variant (NM_173689.7: c.941-3C>T) in the CRB2 gene. The variant was present in a homozygous state in the affected individuals, while in a heterozygous state in phenotypically normal parents. Results: The study expanded the spectrum of the mutations in the gene CRB2 responsible for causing NS. Conclusions: In addition, the study will also help in genetic counseling, carrier testing, and prenatal and/or postnatal early diagnosis of the disease in the affected family.
Keywords: CRB2; nephrotic syndrome; novel splice site variant; whole exome sequencing.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
