

Comparison of Clinical and Radiographic Outcomes According to the Presence or Absence of a Posterior Draw Force during Graft Fixation in Anterior Cruciate Ligament Reconstruction
- PMID: 36556989
- PMCID: PMC9785038
- DOI: 10.3390/medicina58121787
Comparison of Clinical and Radiographic Outcomes According to the Presence or Absence of a Posterior Draw Force during Graft Fixation in Anterior Cruciate Ligament Reconstruction
Abstract
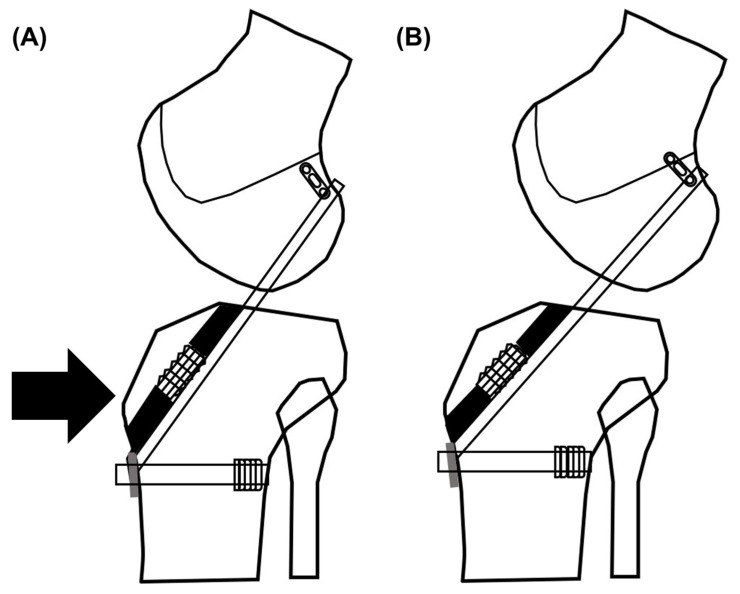
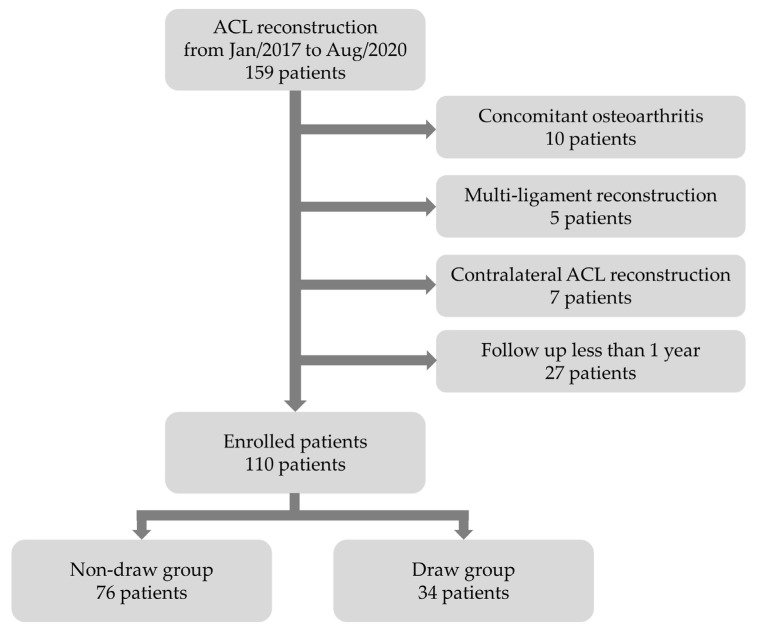
Background and Objectives: A reduction forced toward the posterior side during graft fixation may help to lessen anterior tibial translation after ACL reconstruction. The purpose was to compare the clinical and radiological outcomes of graft fixation when a posterior draw was used and when it was not used during anterior cruciate ligament (ACL) reconstruction surgery. Materials and Methods: Of 110 patients who had undergone primary arthroscopic ACL reconstruction between January 2017 and August 2020, in all, 76 patients had been operated on without a posterior draw (non-draw group), and 34 patients had received surgery with a posterior draw (draw group). The results of the Lachman test and the pivot-shift test, the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) indexes, the Lysholm scores, the International Knee Documentation Committee (IKDC) subjective scores, and side-to-side difference (STSD) on stress radiography were compared between the two groups. Results: The postoperative WOMAC indexes, Lysholm scores, and IKDC subjective scores were similar across both groups. Postoperative STSD (2.4 ± 2.2 for the non-draw group vs. 2.0 ± 2.2 for the draw group; p = 0.319) and change in STSD (3.5 ± 3.5 for preoperative STSD vs. 4.3 ± 4.4 for postoperative STSD; p = 0.295) were not superior in the draw group. Conclusions: The take-home message is that graft fixation with a posterior draw during ACL reconstruction did not result in significantly better postoperative stability. The postoperative clinical outcomes were similar between both groups.
Keywords: anterior cruciate ligament reconstruction; draw; graft.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
-
- Bowers A.L., Bedi A., Lipman J.D., Potter H.G., Rodeo S.A., Pearle A.D., Warren R.F., Altchek D.W. Comparison of anterior cruciate ligament tunnel position and graft obliquity with transtibial and anteromedial portal femoral tunnel reaming techniques using high-resolution magnetic resonance imaging. Arthroscopy. 2011;27:1511–1522. doi: 10.1016/j.arthro.2011.07.007. - DOI - PubMed
-
- Kopf S., Forsythe B., Wong A.K., Tashman S., Anderst W., Irrgang J.J., Fu F.H. Nonanatomic tunnel position in traditional transtibial single-bundle anterior cruciate ligament reconstruction evaluated by three-dimensional computed tomography. J. Bone Jt. Surg. Am. 2010;92:1427–1431. doi: 10.2106/JBJS.I.00655. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
