

The Prevalence of Small Intestinal Bacterial Overgrowth in Patients with Non-Alcoholic Liver Diseases: NAFLD, NASH, Fibrosis, Cirrhosis-A Systematic Review, Meta-Analysis and Meta-Regression
- PMID: 36558421
- PMCID: PMC9783356
- DOI: 10.3390/nu14245261
The Prevalence of Small Intestinal Bacterial Overgrowth in Patients with Non-Alcoholic Liver Diseases: NAFLD, NASH, Fibrosis, Cirrhosis-A Systematic Review, Meta-Analysis and Meta-Regression
Abstract
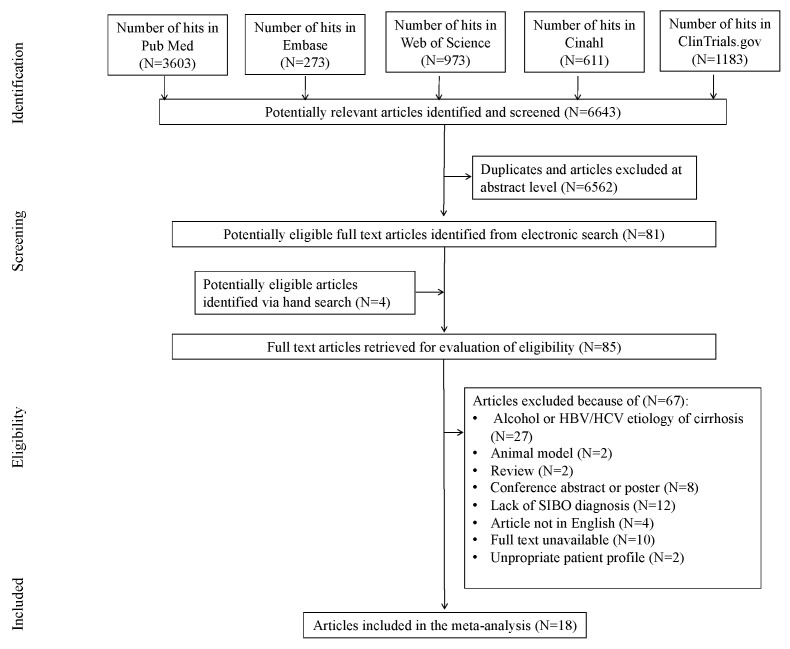
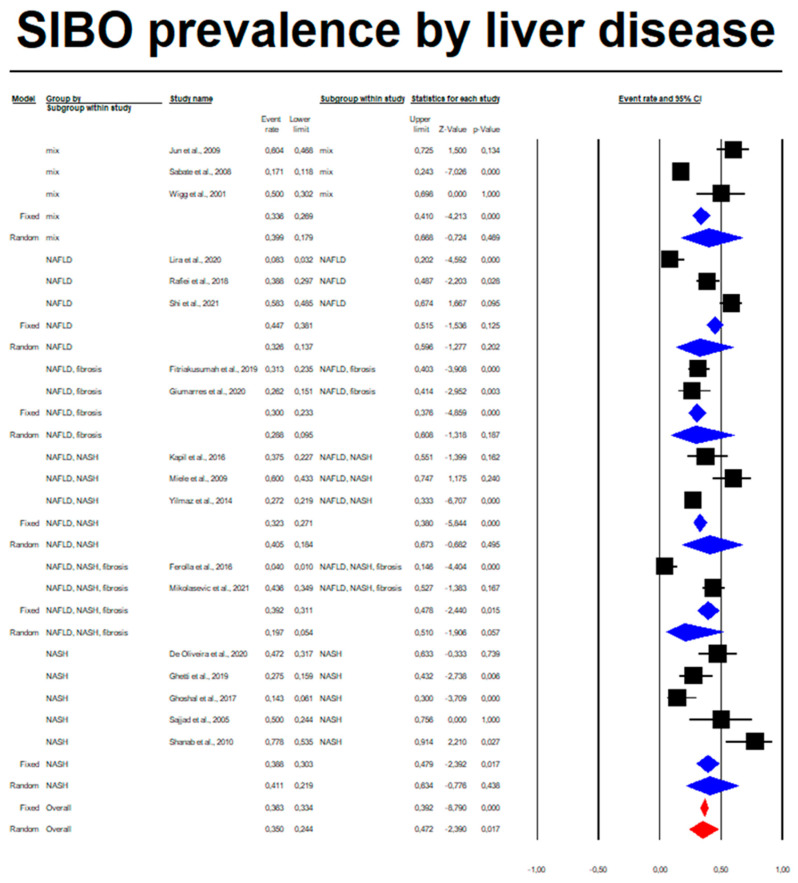
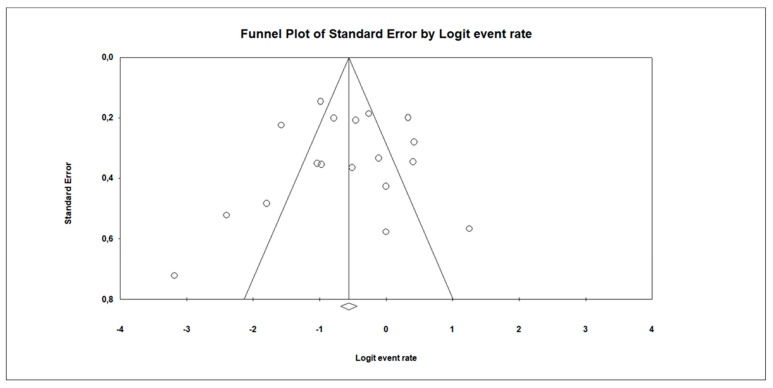
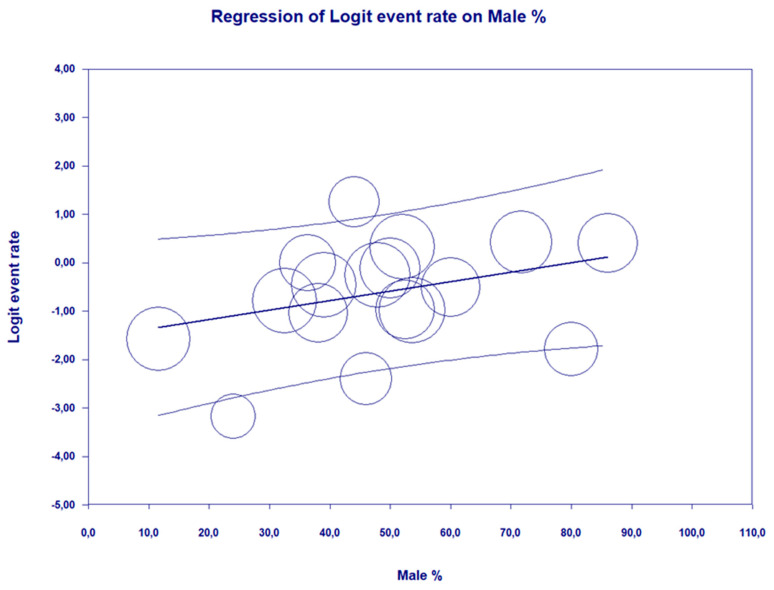
Bacterial overgrowth in the small intestine (SIBO) is a pathological growth of the intestinal microbiota in the small intestine that causes clinical symptoms and can lead to digestive and absorption disorders. There is increasing evidence that people with NAFLD have a distinct gut microflora profile as well metabolome changes compared to people without NAFLD. Thorough analysis of observational and RCT studies in the current databases (EMBASE, Web of Science, PubMed, Cinahl, Clinical Trials) was conducted from 3 November 2021 to 21 June 2022. The following inclusion criteria were applied: confirmed NAFLD, NASH, LIVER FIBROSIS, CIRRHOSIS due to steatosis; diagnostic methods of liver diseases—biopsy, elastography, transabdominal ultrasound; nonalcoholic fatty liver disease activity score; confirmed SIBO; diagnostic methods of SIBO−breath tests (hydrogen test; methane test and mix test; duodenal and jejunal aspiration before any type of intervention; adults above 18yo; number of participants ≥20; full articles. We excluded review articles, populations with HBV/HCV infection and alcohol etiology and interventions that may affect NAFLD or SIBO treatment. The quality of each study methodology was classified by means of the Cochrane Collaboration’s tool (RCT) and Newcastle—Ottawa Quality Assessment Scale adapted for cross-sectional, cohort and case-control studies. The random effects meta-analysis of outcomes for which ≥2 studies contributed data was conducted. The I2 index to measure heterogeneity and the χ2 test of homogeneity (statistically significant heterogeneity p < 0.05) were applied. For categorical outcome, the pooled event rate (effect size) was calculated. This systematic review was reported according to PRISMA reporting guidelines. We initially identified 6643 studies, from which 18 studies were included in final meta-analysis. The total number of patients was 1263. Accepted SIBO diagnostic methods were both available breath tests (n-total = 15) and aspirate culture (n-total = 3). We found that among patients with non-alcoholic liver diseases, the random overall event rate of SIBO was 0.350 (95% CI, 0.244−0.472), p = 0.017. The subgroup analysis regarding a type of diagnosis revealed that the lowest ER was among patients who developed simultaneously NAFLD, NASH and fibrosis: 0.197 (95% CI, 0.054−0.510) as compared to other annotated subgroups. The highest prevalence of SIBO was observed in the NASH subgroup: 0.411 (95% CI, 0.219−0.634). There were no statistically significant differences in the prevalence of SIBO in different subgroups (p = 0.854). Statistically significant heterogeneity between studies was estimated (I2 = 86.17%, p = 0.00). Egger’s test did not indicate a publication bias (df = 16, p = 0.885). A meta-regression using a random-effects model revealed that higher percentage of males in the population with liver diseases is a predisposing factor toward SIBO (Q = 4.11, df = 1, p = 0.0426 with coefficient = 0.0195, SE = 0.0096, Z = 2.03). We showed that the prevalence of SIBO in patients with chronic non-alcoholic liver diseases can be as high as 35%, and it increases with the percentage of men in the population. The prevalence of SIBO does not differ significantly depending on the type of chronic liver disease. Despite the high heterogeneity and moderate and low quality of included studies, our meta-analysis suggests the existence of a problem of SIBO in the population of patients with non-alcoholic liver diseases, and the presence of SIBO, in turn, determines the therapeutic treatment of such type of patients, which indicates the need for further research in this area. The study protocol was registered with the international Prospective Register of Systematic Reviews (PROSPERO ID: CRD42022341473).
Keywords: NAFLD; NASH; cirrhosis; gut dysbiosis; microbiome; small intestinal bacterial overgrowth; steatosis.
Conflict of interest statement
The authors declare no conflict of interest. A.G., D.J.-M., V.H., K.S.-Ż., E.S.—no competing interest declared. All authors have read and approved the final manuscript.
Figures
Similar articles
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Interventions for the treatment of brain radionecrosis after radiotherapy or radiosurgery.Cochrane Database Syst Rev. 2018 Jul 9;7(7):CD011492. doi: 10.1002/14651858.CD011492.pub2. Cochrane Database Syst Rev. 2018. PMID: 29987845 Free PMC article.
-
Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Feb 24;2(2):CD013556. doi: 10.1002/14651858.CD013556.pub2. Cochrane Database Syst Rev. 2022. PMID: 35199850 Free PMC article.
-
Sertindole for schizophrenia.Cochrane Database Syst Rev. 2005 Jul 20;2005(3):CD001715. doi: 10.1002/14651858.CD001715.pub2. Cochrane Database Syst Rev. 2005. PMID: 16034864 Free PMC article.
-
Selenium for preventing cancer.Cochrane Database Syst Rev. 2018 Jan 29;1(1):CD005195. doi: 10.1002/14651858.CD005195.pub4. Cochrane Database Syst Rev. 2018. PMID: 29376219 Free PMC article.
Cited by
-
Helicobacter pylori infection and small intestinal bacterial overgrowth: a systematic review and meta-analysis.BMC Microbiol. 2023 Dec 6;23(1):386. doi: 10.1186/s12866-023-03063-w. BMC Microbiol. 2023. PMID: 38053022 Free PMC article.
-
Evaluation and Management of Nutritional Consequences of Chronic Liver Diseases.Nutrients. 2023 Aug 7;15(15):3487. doi: 10.3390/nu15153487. Nutrients. 2023. PMID: 37571424 Free PMC article. Review.
-
Genetic predisposition of the gastrointestinal microbiome and primary biliary cholangitis: a bi-directional, two-sample Mendelian randomization analysis.Front Endocrinol (Lausanne). 2023 Oct 12;14:1225742. doi: 10.3389/fendo.2023.1225742. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37900141 Free PMC article.
-
Epidemiology of small intestinal bacterial overgrowth.World J Gastroenterol. 2023 Jun 14;29(22):3400-3421. doi: 10.3748/wjg.v29.i22.3400. World J Gastroenterol. 2023. PMID: 37389240 Free PMC article. Review.
-
Recurrent Clostridioides difficile Infection (CDI) in Patients Treated With Vancomycin at Johns Hopkins Aramco Healthcare (JHAH), Dhahran, Saudi Arabia.Cureus. 2025 May 31;17(5):e85116. doi: 10.7759/cureus.85116. eCollection 2025 May. Cureus. 2025. PMID: 40599506 Free PMC article.
References
-
- Shindo K., Machida M., Miyakawa K., Fukumura M. A Syndrome of Cirrhosis, Achlorhydria, Small Intestinal Bacterial Overgrowth, and Fat Malabsorption. Am. J. Gastroenterol. 1993;88:2084–2091. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
