

Use of Robot-Assisted Gait Training in Pediatric Patients with Cerebral Palsy in an Inpatient Setting-A Randomized Controlled Trial
- PMID: 36560316
- PMCID: PMC9783925
- DOI: 10.3390/s22249946
Use of Robot-Assisted Gait Training in Pediatric Patients with Cerebral Palsy in an Inpatient Setting-A Randomized Controlled Trial
Abstract
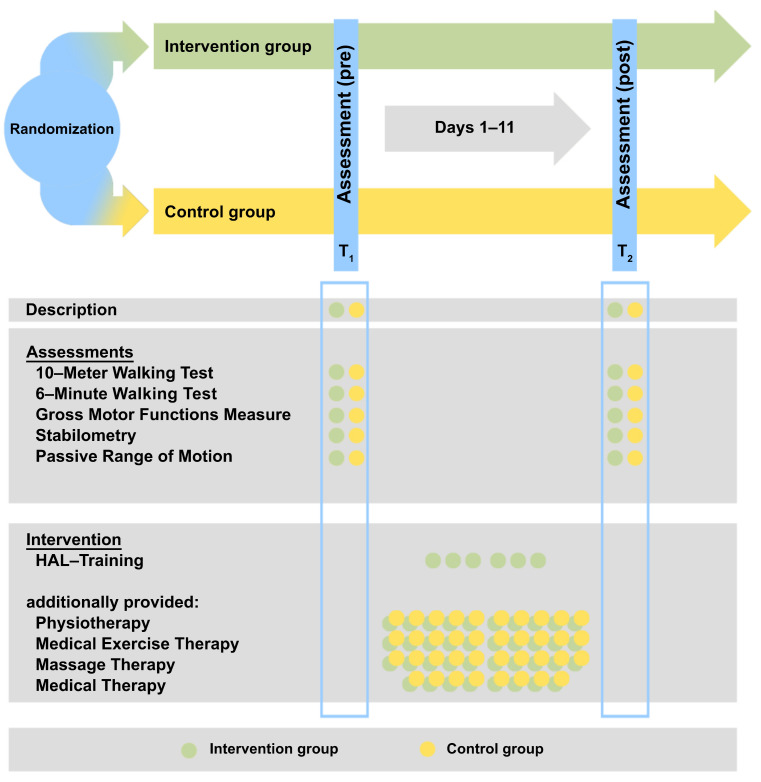
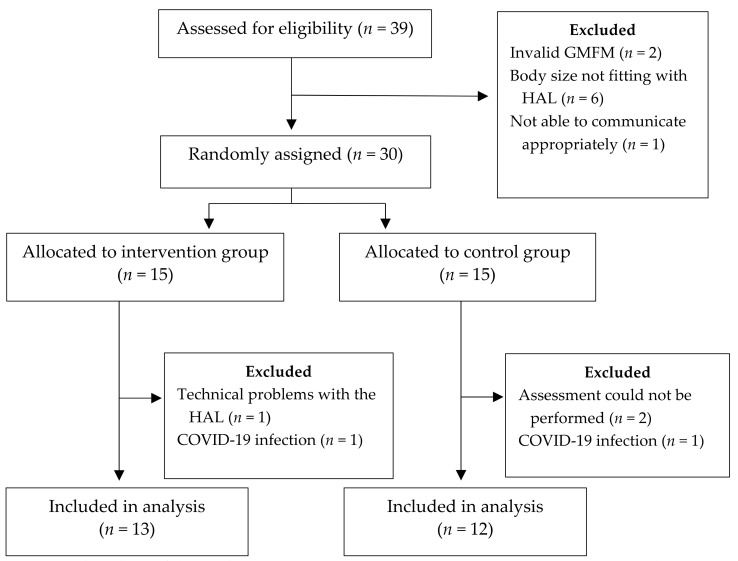
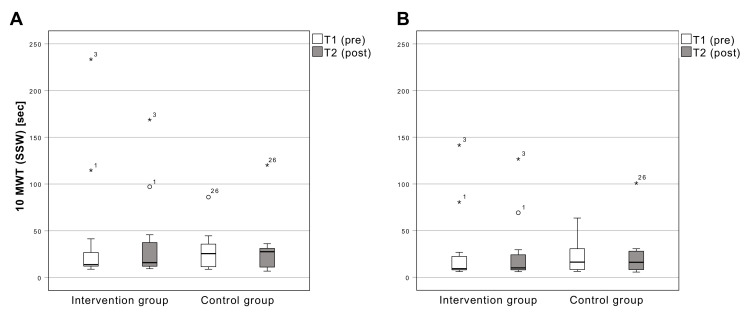
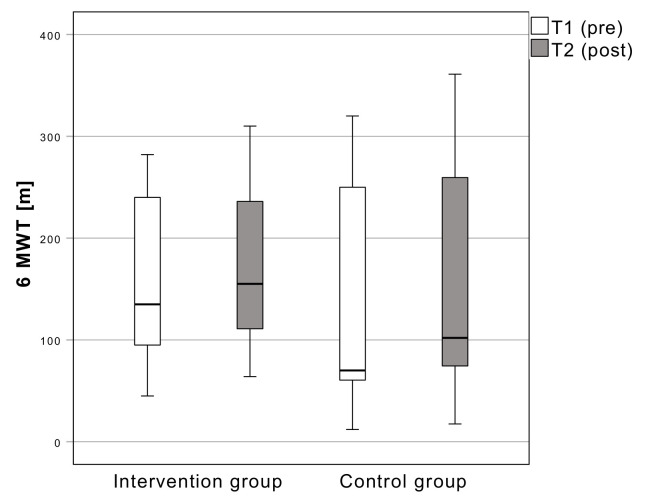
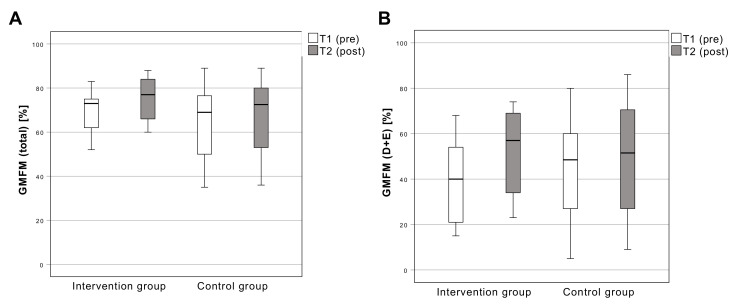
Robot-assisted gait training (RAGT) provides a task-based support of walking using exoskeletons. Evidence shows moderate, but positive effects in the therapy of patients with cerebral palsy (CP). This study investigates the impact of RAGT on walking speed and gait parameters in pediatric CP patients. Thirty subjects (male = 23; female = 7), with a mean age of 13.0 ± 2.5 (9-17) years, and with spastic CP, were recruited. The intervention group (n = 15) underwent six 20-minute RAGT sessions with the Hybrid Assistive Limb (HAL) during an 11-day hospital stay. Additionally, a therapy concept including physiotherapy, physician-performed manual medicine, massage and exercise therapy was provided. The control group (n = 15) was treated with the therapy concept only. The outcome was based on a 10-Metre Walking Test (10MWT), 6-Minute Walking Test (6MWT), Gross Motor Function Measure (GMFM-88) and lower extremities passive range of motion. The intervention group achieved a mean increase in walking speed in the 10MWT (self-selected walking speed SSW) of 5.5 s (p = 0.378). There were no significant differences between the groups in the 10MWT (max) (p = 0.123) and the 6MWT (p = 0.8). Changes in the GMFM (total) and in the dimension standing and walking, running and jumping (D + E) showed clinically relevant significant results (p = 0.002 and p = 0.046). RAGT as a supplement to an inpatient therapy stay appears to have a positive, yet not significant impact on the gait parameters of pediatric CP patients as well as motivating them to practice walking. Further studies with adapted study designs are needed to evaluate different influencing factors.
Keywords: cerebral palsy; exoskeleton device; gait disorders neurologic; hybrid assistive limb; pediatrics; robot-assisted gait training; walk test; walking.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Figures
References
-
- Gage J.R. Gait Pathology in Individuals with Cerebral Palsy. In: Gage J.R., Schwartz M.H., Koop S.E., editors. The Identification and Treatment of Gait Problems in Cerebral Palsy. Mac Keith Press; London, UK: 2009. pp. 11–171.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
